ABSTRACT
Burning mouth syndrome is an enigmatic condition that can be difficult to recognize and diagnose. Dental practitioners must be able to distinguish between primary (essential or idiopathic) and secondary burning mouth syndrome. The primary form is characterized by a burning sensation in the oral mucosa and perioral areas, typically with bilateral, symmetric distribution and an absence of relevant clinical and laboratory findings. In the secondary form, the burning sensation is due to clinical abnormalities or a systemic or psychological condition. To date, primary burning mouth syndrome has been considered a diagnosis of exclusion. A case description of a woman with oral burning sensations and the results of a retrospective case analysis are presented to aid practitioners in the understanding, recognition and diagnosis of primary burning mouth syndrome.
Introduction
A 51-year-old woman presented to a dental office with bilateral oral burning sensation on the anterior dorsum of the tongue, the anterior aspect of the hard palate and the mandibular lip. She stated that the oral burning began spontaneously about 10 years ago but was unable to recall any precipitating event. She described the burning sensation as constant, accompanied by numbness and tingling, with an average intensity rating of 8 (on a scale of 0 [no pain] to 10 [pain as bad as it can be]). She reported that the sensation typically worsened as the day progressed. More generally, the intensity of the burning sensation had increased over time since initial onset. The patient stated that the burning increased with stress and consumption of hot liquids, but decreased when she was eating. Additionally, she complained of dry mouth and a constant salty taste, regardless of oral intake. The burning did not affect her sleep pattern. She was perimenopausal and reported diagnoses of fibromyalgia, depression and hypertension. She was taking an antidepressant, an anticonvulsant and an antihypertensive medication for these existing medical conditions. Her dental history was unremarkable. A variety of diagnostic tests had been performed previously to rule out local conditions (mucosal lesions, dental disease and infectious conditions such as fungal or viral infections), as well as systemic conditions (endocrine disorders such as diabetes mellitus and hypothyroidism, nutritional disorders, anemia and central nervous system pathology). These previous diagnostic tests included routine dental and medical imaging studies (computed tomography, magnetic resonance imaging), hematological screening, allergy testing and biopsy of the oral mucosa, but the results of all of these investigations had been unremarkable and did not point to any underlying cause of the burning sensation. She denied use of nicotine products, ethanol or recreational drugs, and she reported no parafunctional habits.
Examination, including palpation, revealed no abnormalities of the extraoral structures (cranial nerves, lymph nodes, muscles, joints) or the intraoral structures (oral mucosa and tongue, dentition, periodontal tissues, existing restorations). The cervical range of movement was without limitation, and movement of the cervical spine did not reproduce her chief complaint.
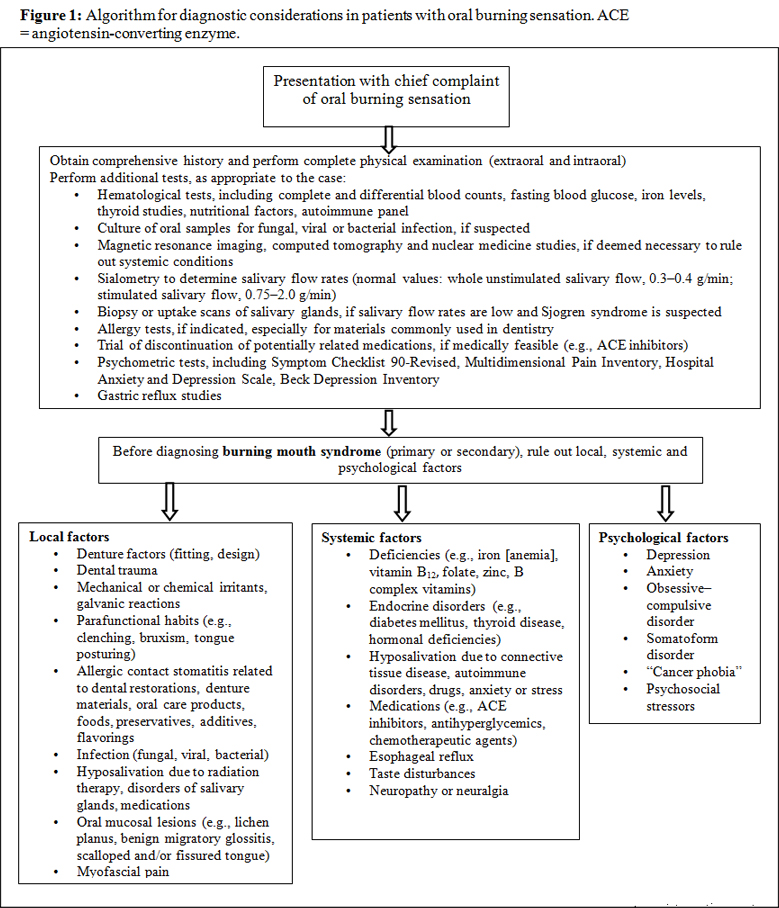
This patient had clinical characteristics that were consistent with a diagnosis of burning mouth syndrome. The primary (essential or idiopathic) form of this condition is characterized by a burning sensation in the oral mucosa and perioral areas, typically with a bilateral and symmetric distribution and an absence of relevant clinical and laboratory findings to account for the burning.1-3 The diagnosis requires recognizing the symptoms and their characteristics and ruling out underlying oral and/or systemic disease, with adjunctive use of laboratory studies and/or imaging as appropriate (Fig. 1). As such, primary burning mouth syndrome is a diagnosis of exclusion.
Retrospective Analysis of Previous Cases
The challenge of reaching a definitive diagnosis in this case suggested that it might be beneficial to review previous cases involving oral burning sensation. Therefore, the goal of this review was to identify any patterns that would aid in reaching the definitive diagnosis, thereby leading, in turn, to appropriate management strategies.
A retrospective analysis of cases from an oral medicine/orofacial pain clinic was undertaken, with approval from the University of Illinois at Chicago Institutional Review Board. Records were retrieved for 49 consecutive adult patients (18 years of age or older) who presented with oral burning sensation over a 5-year period (January 2003 to March 2008). Most of the patients (43 or 88%) were women, and most were in their 50s (mean age 56.4 years, range 33 to 68 years). In each case, 1 of 2 clinicians (GDK or JBE) obtained a complete history, performed a thorough examination, completed hematological screening (complete and differential blood counts, fasting blood glucose, iron, vitamin B complex, folate and thyroid function), performed sialometry (i.e., determination of weight of stimulated and unstimulated whole saliva) and evaluated the patient for diseases related to salivary gland hypofunction, with laboratory testing for autoimmune and connective tissue diseases, before reaching the definitive diagnosis, in accordance with the diagnostic approach detailed in Fig. 1.
The site of the “worst” sensation of burning among the patients in the retrospective study (tongue > lips > hard palate) was slightly different from that reported by the patient (tongue > hard palate > lip) described in the current case report, but was generally consistent with findings from the literature, with the pain often occurring at multiple sites.4-7 Like the patient in the current case report, most of those in the retrospective study reported the onset of oral burning as “sudden” (35 or 76%; data not available for 3 patients) rather than “gradual” (11 or 24%; data not available for 3 patients), and as “constant” (39 or 80%) as opposed to either “intermittent” (9 or 18%) or “other” (1 or 2%). The patient in the case reported here described the oral burning in typical terms, with the burning sensation having a significant negative impact on her quality of life.1 The reported 10-year duration of symptoms in this case concurred with the literature, which has documented durations of months to years, with or without periods of cessation or remission.8 The intensity of oral burning is often described as moderate to severe, and the severity (but not quality) of the sensation is sometimes referred to as comparable to that of toothache pain.9 Similar to the patient in the current case report and as reported in the literature,8,10,11 the majority of patients in the retrospective study (30 or 63%; data not available for 1 patient) indicated that the intensity of burning had increased since initial onset; only 3 patients (6%; data not available for 1 patient) reported a decrease in symptoms over time, and 15 (31%; data not available for 1 patient) reported no change. Generally, patients are unaware of oral burning during sleep or upon waking, with the sensations gradually increasing to peak intensity in late afternoon and early evening.1,2 Overall then, the patient described in the current case report shared many characteristics with patients in the retrospective study and in other reports in the literature.
Many of the patients in the retrospective study reported that the onset of the burning sensation was related to an identifiable event such as dental treatment (13 or 27%), administration of a new medication (8 or 16%) or some other medical or personal event (7 or 14%), but none specifically reported stressors as a precipitator of their condition. The remaining 21 patients (43%) reported that the precipitating event was unknown. The literature suggests that about 17% to 33% of patients attribute the onset of symptoms to an upper respiratory tract infection, previous dental procedure or medication use (including antibiotic therapy),8,12,13 whereas others claim that the onset of symptoms is related to traumatic life stressors.6,8,10 The patient in the current case was unable to recall any precipitating event but did have several medical conditions that could have psychological overtones (e.g., depression). Similar to this patient, dry mouth (reported by 30 or 61%) and taste disturbances (taste alteration and/or change in taste intensity, reported by 26 or 53%) were common in the retrospective study. These characteristics are common among individuals with oral burning sensations, both experimentally and clinically2,4,5,14-20 and may be equally or more disturbing than the oral burning itself.2 The literature also suggests that in some cases, oral burning decreases or is abolished upon oral intake or stimulation,2 as was reported by the patient in the current case report. This feature was reported by only a minority of patients in the retrospective study (4 or 8%), whereas the majority reported either a paradoxical effect of increased oral burning (20 or 41%) or no change (25 or 51%) upon oral intake or stimulation. The relationship among taste function, oral intake and oral burning requires further investigation.
The patients in the retrospective study, like the patient in the case report, typically had coexisting medical conditions (Table 1). It is possible that these systemic conditions or certain medications used to treat them may have precipitated or contributed to the patients’ symptoms, as indicated in the literature.21-28 Many individuals with oral burning have had more nonspecific health complaints and more severe menopausal symptoms than healthy controls.4
Table 1 Medical conditions reported by patients at the time of presentation
| Medical condition | No. (%) of patientsa (n = 49) |
| Hypertension | 16 (33) |
| Gastroesophageal reflux disease | 14 (29) |
| Hypercholesterolemia | 11 (22) |
| Autoimmune disorder | 11 (22) |
| Thyroid disorder | 7 (14) |
| Anemia | 1 (2) |
a Some patients reported more than one condition.
Discussion
From a clinical perspective, the etiology of primary burning mouth syndrome is not well defined. As such, the treatment options that are typically considered are based upon patients’ symptoms. In contrast, in cases of secondary burning mouth syndrome, where the oral burning is due to clinical abnormalities or systemic and/or psychological conditions, diagnosis and treatment of the underlying condition should be pursued.
The prevalence of burning mouth syndrome is between 0.7% and 5% of the general population (including Canadian studies2,10). The variation in prevalence is likely related to study methodology (survey versus clinical assessment) and geographic location.2,4,19,29 Burning mouth syndrome is most commonly reported by women in their 50s through 70s4,30,31 and usually presents from 3 years before to 12 years after menopause.4 The condition is rare in patients under the age of 30 years.18,32 The reported sex ratio of affected patients (females to males) has ranged from 3:1 to 16:1.4,6,33-35 Extrapolating these data to the Canadian population, burning mouth syndrome may affect between 250 000 and 1.5 million Canadians.
There is an increasing consensus that burning mouth syndrome is an idiopathic neuropathic pain condition.30,36 Recent evidence has suggested both central37-40 and peripheral31,41-43 neuropathic changes. Damage to taste has also been reported in association with burning mouth syndrome, because of disinhibition of pain signalling.44 In addition, an etiological theory regarding steroid dysregulation in patients with this condition has been proposed.45
Patients such as the one described in this case report may present to the dental office with a distinct set of clinical characteristics common to those with burning mouth syndrome. It is incumbent upon dental practitioners to be able to recognize these often overlooked and misinterpreted presentations. In so doing, they should be able to develop a working diagnosis. However, if in doubt, dental practitioners should refer these enigmatic cases to colleagues with advanced training in oral medicine and orofacial pain, because of the need to assess a broad range of oral and systemic factors. The management of all chronic pain conditions, including burning mouth syndrome, has the goal of improving symptom control and, ideally, resolving the condition, but the process may be complex. Considerations for management of burning mouth syndrome are discussed in an accompanying article.46
THE AUTHORS
|
Dr. Klasser is associate professor, Louisiana State University School of Dentistry, New Orleans, LA. |
|
|
Dr. Epstein is professor, University of Illinois at Chicago, College of Dentistry, department of oral medicine and diagnostic sciences; director, interdisciplinary program in oral cancer biology, prevention and treatment, College of Medicine, Chicago Cancer Center, Chicago, IL. |
|
|
Ms. Villines is research coordinator, Advocate Lutheran General, Park Ridge, IL. |
Correspondence to: Dr. Gary D. Klasser, Louisiana State University School of Dentistry, Division of diagnostic sciences, 1100 Florida Ave., New Orleans, LA 70119, USA. Email: gklass@lsuhsc.edu.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- Woda A, Navez ML, Picard P, Gremeau C, Pichard-Leandri E. A possible therapeutic solution for stomatodynia (burning mouth syndrome). J Orofac Pain. 1998;12(4):272-8.
- Grushka M, Epstein JB, Gorsky M. Burning mouth syndrome. Am Fam Physician. 2002;65(4):615-20.
- Danhauer SC, Miller CS, Rhodus NL, Carlson CR. Impact of criteria-based diagnosis of burning mouth syndrome on treatment outcome. J Orofac Pain. 2002;16(4):305-11.
- Grushka M. Clinical features of burning mouth syndrome. Oral Surg Oral Med Oral Pathol. 1987;63(1):30-6.
- Gorsky M, Silverman S Jr, Chinn H. Burning mouth syndrome: a review of 98 cases. J Oral Med. 1987;42(1):7-9.
- van der Ploeg HM, van der Wal N, Eijkman MA, van der Waal I. Psychological aspects of patients with burning mouth syndrome. Oral Surg Oral Med Oral Pathol. 1987;63(6):664-8.
- Svensson P, Bjerring P, Arendt-Nielsen L, Kaaber S. Sensory and pain thresholds to orofacial argon laser stimulation in patients with chronic burning mouth syndrome. Clin J Pain. 1993;9(3):207-15.
- Grushka M, Katz RL, Sessle BJ. Spontaneous remission in burning mouth syndrome. J Dent Res. 1987;66:274.
- Grushka M, Sessle BJ, Miller R. Pain and personality profiles in burning mouth syndrome. Pain. 1987;28(2):155-67.
- Grushka M, Sessle BJ. Burning mouth syndrome. Dent Clin North Am. 1991;35(1):171-84.
- Drage LA, Rogers RS 3rd. Clinical assessment and outcome in 70 patients with complaints of burning or sore mouth symptoms. Mayo Clin Proc. 1999;74(3):223-8.
- Tammiala-Salonen T, Hiidenkari T, Parvinen T. Burning mouth in a Finnish adult population. Community Dent Oral Epidemiol. 1993;21(2):67-71.
- Hammaren M, Hugoson A. Clinical psychiatric assessment of patients with burning mouth syndrome resisting oral treatment. Swed Dent J. 1989;13(3):77-88.
- Maresky LS, van der Bijl P, Gird I. Burning mouth syndrome. Evaluation of multiple variables among 85 patients. Oral Surg Oral Med Oral Pathol. 1993;75(3):303-7.
- Nilner K, Nilsson B. Intraoral currents and taste thresholds. Swed Dent J. 1982;6(3):105-13.
- Ship JA, Grushka M, Lipton JA, Mott AE, Sessle BJ, Dionne RA. Burning mouth syndrome: an update. J Am Dent Assoc. 1995;126(7):842-53.
- Grushka M, Sessle B. Taste dysfunction in burning mouth syndrome. Gerodontics. 1988;4(5):256-8.
- Bergdahl M, Bergdahl J. Burning mouth syndrome: prevalence and associated factors. J Oral Pathol Med. 1999;28(8):350-4.
- Eguia Del Valle A, Aguirre-Urizar JM, Martinez-Conde R, Echebarria-Goikouria MA, Sagasta-Pujana O. Burning mouth syndrome in the Basque Country: a preliminary study of 30 cases. Med Oral. 2003;8(2):84-90.
- Grushka M, Sessle BJ, Howley TP. Psychophysical evidence of taste dysfunction in burning mouth syndrome. Chem Senses. 1986;11(4):485-98.
- Netto FO, Diniz IM, Grossmann SM, de Abreu MH, do Carmo MA, Aguiar MC. Risk factors in burning mouth syndrome: a case-control study based on patient records. Clin Oral Investig. 2010 May 4. [Epub ahead of print].
- Femiano F, Lanza A, Buonaiuto C, Gombos F, Nunziata M, Cuccurullo L, et al. Burning mouth syndrome and burning mouth in hypothyroidism: proposal for a diagnostic and therapeutic protocol. Oral Surg Oral Med Oral Pathol. 2008;105(1):e22-7.
- Soares MS, Chimenos-Kustner E, Subira-Pifarre C, Rodriguez de Rivera-Campillo ME, Lopez-Lopez J. Association of burning mouth syndrome with xerostomia and medicines. Med Oral Patol Oral Cir Bucal. 2005;10(4):301-8.
- Salort-Llorca C, Minguez-Serra MP, Silvestre FJ. Drug-induced burning mouth syndrome: a new etiological diagnosis. Med Oral Patol Oral Cir Bucal. 2008;13(3):E167-70.
- Brailo V, Vueiaeeviae-Boras V, Alajbeg IZ, Alajbeg I, Lukenda J, Aeurkoviae M. Oral burning symptoms and burning mouth syndrome-significance of different variables in 150 patients. Med Oral Patol Oral Cir Bucal. 2006;11(3):E252-5.
- Di Fede O, Di Liberto C, Occhipinti G, Vigneri S, Lo Russo L, Fedele S, and others. Oral manifestations in patients with gastro-oesophageal reflux disease: a single-center case-control study. J Oral Pathol Med. 2008;37(6):336-40 Epub 2008 Feb 15.
- Gao J, Chen L, Zhou J, Peng J. A case-control study on etiological factors involved in patients with burning mouth syndrome. J Oral Pathol Med. 2009;38(1):24-8.
- Carrington J, Getter L, Brown RS. Diabetic neuropathy masquerading as glossodynia. J Am Dent Assoc. 2001;132(11):1549-51.
- Klausner JJ. Epidemiology of chronic facial pain: diagnostic usefulness in patient care. J Am Dent Assoc. 1994;125(12):1604-11.
- Zakrzewska JM. The burning mouth syndrome remains an enigma. Pain. 1995;62(3):253-7.
- Lauria G, Majorana A, Borgna M, Lombardi R, Penza P, Padovani A, et al. Trigeminal small-fiber sensory neuropathy causes burning mouth syndrome. Pain. 2005;115(3):332-7.
- van der Waal I. The burning mouth syndrome. Copenhagen: Munksgaard; 1990. p. 5-90.
- Basker RM, Sturdee DW, Davenport JC. Patients with burning mouths. A clinical investigation of causative factors, including the climacteric and diabetes. Br Dent J. 1978;145(1):9-16.
- Main DM, Basker RM. Patients complaining of a burning mouth. Further experience in clinical assessment and management. Br Dent J. 1983;154(7):206-11.
- Gorsky M, Silverman S Jr, Chinn H. Clinical characteristics and management outcome in the burning mouth syndrome. An open study of 130 patients. Oral Surg Oral Med Oral Pathol. 1991;72(2):192-5.
- Patton LL, Siegel MA, Benoliel R, De Laat A. Management of burning mouth syndrome: systematic review and management recommendations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103 Suppl:S39 e1-13.
- Jaaskelainen SK, Rinne JO, Forssell H, Tenovuo O, Kaasinen V, Sonninen P, et al. Role of the dopaminergic system in chronic pain -- a fluorodopa-PET study. Pain. 2001;90(3):257-60.
- Jaaskelainen SK. Clinical neurophysiology and quantitative sensory testing in the investigation of orofacial pain and sensory function. J Orofac Pain. 2004;18(2):85-107.
- Hagelberg N, Forssell H, Aalto S, Rinne JO, Scheinin H, Taiminen T, et al. Altered dopamine D2 receptor binding in atypical facial pain. Pain. 2003;106(1-2):43-8.
- Forssell H, Jaaskelainen S, Tenovuo O, Hinkka S. Sensory dysfunction in burning mouth syndrome. Pain. 2002;99(1-2):41-7.
- Heckmann SM, Heckmann JG, HiIz MJ, Popp M, Marthol H, Neundorfer B, et al. Oral mucosal blood flow in patients with burning mouth syndrome. Pain. 2001;90(3):281-6.
- Formaker BK, Mott AE, Frank ME. The effects of topical anesthesia on oral burning in burning mouth syndrome. Ann N Y Acad Sci. 1998;855:776-80.
- Nagler RM, Hershkovich O. Sialochemical and gustatory analysis in patients with oral sensory complaints. J Pain. 2004;5(1):56-63.
- Grushka M BL. Burning mouth syndrome and oral dysesthesias. Can J Diagnosis. 2000;17(6):99-109.
- Woda A, Dao T, Gremeau-Richard C. Steroid dysregulation and stomatodynia (burning mouth syndrome). J Orofac Pain. 2009;23(3):202-10.
- Klasser GD, Epstein JB, Villines D. Management of burning mouth syndrome. J Can Dent Assoc. 2011;77:b151.