
Abstract
Background: Accurate determination of the apical terminus plays a significant role in the success of root canal therapy, but accuracy may be affected by the presence of accessory canals.
Objective: To evaluate the accuracy of a ratio-based electronic apex locator for roots with simulated lateral canals.
Methods: Forty-two single-rooted human teeth were randomly divided into 2 groups. For each tooth, the root canal was prepared to the visually determined working length, and the working length was then measured with the Justy II electronic apex locator. Simulated lateral canals (of 2 different diameters) were then prepared at 3 mm (group A) or 6 mm (group B), and the working lengths were measured again with the same instrument. The measurements were analyzed by one-way analysis of variance.
Results: For both groups, there were no significant changes in working length after the creation of simulated canals (p > 0.05).
Conclusion: Measurements obtained with the ratio-based electronic apex locator were not affected by the preparation of simulated lateral canals, and the instrument was able to accurately determine the location of the tooth apex.
Accurate determination of the apical terminus (major foramen or apex) plays a significant role in the success of root canal therapy, specifically in calculating the working length. Working length is defined as "the distance from a coronal reference point to the point at which canal preparation and filling should terminate." 1 Several techniques, including electronic methods, have been used to determine the position of the apex.2 Electronic apex locators detect the canal terminus using certain characteristics of human tissues that can be modelled by a combination of electrical components.2 However, in some cases, the device incorrectly indicates that the apex has been reached before the instrument tip reaches the apical terminus.3,4 Such inaccuracies may be caused by extensive carious lesions or metallic restorations or, in the absence of disease or restoration, a vertical fissure, fracture, root perforation or accessory canal.
An accessory canal is any branch of the main pulp canal or chamber that communicates with the external surface of the root.5 A lateral canal is an accessory canal located in the coronal or middle third of the root, usually extending horizontally from the main root canal.5 It has been shown that accessory canals are present in a substantial percentage of teeth.6 For example, De Deus6 found lateral canals in 27.4% of 1140 teeth and observed that 17% of these lateral canals were located in the apical third of the tooth. A lateral canal forms a 2-way passage between the root canal space and the periodontal tissue.
Previous studies have evaluated the accuracy of electronic apex locators in cases of fracture or perforation,3,4,7 but the effects of lateral canals, whether simulated or real, on the accuracy of these devices have not yet been evaluated. The aim of this study was to evaluate the behaviour and accuracy of a "ratio-based" electronic apex locator in roots with simulated lateral canals.
Methods
Sample Preparation
Forty-two freshly extracted single-rooted human teeth (maxillary incisors and mandibular premolars), with mature apices, single root canals that were both patent and straight, and no cracks or perforations, were selected. A bur was used to decoronate each tooth at the cementoenamel junction, to generate a flat, horizontal surface. The teeth were cleaned, and access cavities were created. The working length of each tooth was first measured visually. A size 10 stainless steel file (VDW, Antaeos, Germany) was inserted into the root canal until the tip of the file reached the plane of the major foramen, as described by Thomas and colleagues.8 The working length was determined by placing the stopper of the file adjacent to the horizontal surface of the root, where the file tip could be seen at the major foramen. The distance between the file tip and the stopper was measured (to 0.02-mm accuracy) with a digital caliper. Each measurement was repeated 3 times, and the average of these 3 measurements was taken as the "raw length." From this value, 0.5 mm was subtracted, and the calculated value was considered the true working length for the purpose of preparing the root canals.
The crown-down technique with stainless steel hand files was used to prepare all root canals to the true working length as determined visually; the master apical file was size 45/0.02 for all roots. The root canals were irrigated with 2.25% sodium hypochlorite (NaOCl) solution during use and during changes of instruments.
After preparation, the 42 roots were randomly divided into 2 groups of 21, designated groups A and B. In both groups, the working length of each root was measured with the electronic apex locator, as described below. These results were recorded as the true working lengths (control).
Normal saline (0.9% sodium chloride) (Vacoliter, Eczacıbaşı, Turkey) was used as a medium for in vitro assessments of the electronic apex locator. For each tooth, a sample of the medium was placed in a glass tube with a tight-fitting rubber seal (Fig. 1). Two openings were made in the rubber seal, one in the centre, for placement of the sample tooth, and the other between the centre and the side of the tube, for placement of the lip electrode of the electronic apex locator. The canal of the tooth was filled with 2.25% NaOCl solution (Fig. 1), and both the lip electrode and the sample tooth were placed in contact with the medium. A size 40 file was then connected to the electrode for electronic measurement of the apex. All measurements were performed by one researcher, under the same experimental conditions, using a single electronic apex locator (Justy II, Toesco, Japan) with 0.5-mm accuracy.
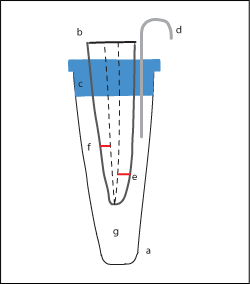 Figure 1: Experimental set-up. a = glass tube, b = sample tooth, c = tightly closed rubber seal, d = lip electrode, e = simulated lateral canal at 3 mm, f = simulated lateral canal at 6 mm, g = sodium chloride solution (0.9%) used as medium.
Figure 1: Experimental set-up. a = glass tube, b = sample tooth, c = tightly closed rubber seal, d = lip electrode, e = simulated lateral canal at 3 mm, f = simulated lateral canal at 6 mm, g = sodium chloride solution (0.9%) used as medium.
Preparation of Simulated Lateral Canals
In group A, each of the 21 roots was measured with a digital ruler, and a mark was made on the mesial surface at 3 mm from the end of the root. A size 15 (0.15 mm at D0 [first millimetre of the tip], with 0.02 mm taper) engine reamer (Dentsply Maillefer, Birmingham, UK) was used to drill into the centre of the canal to prepare the simulated lateral canal. To control the patency of the simulated lateral canal, the master apical file was placed into the main root canal, and the reamer used to make the simulated lateral canal was then connected to the electronic apex locator and repositioned in the lateral canal. When the tip of the reamer contacted the file in the main root canal, the electrical circuit was completed and the device indicated "apex" before the file tip in the root canal reached the actual apex. The working length of each of the 21 roots with a simulated lateral canal was measured and recorded as the "A1" length. Then, the simulated canal was enlarged with a size 20 (0.20 mm at D0, with 0.02 mm taper) engine reamer (Dentsply Maillefer) into the centre of the canal, and the working length of each root was measured again and recorded as the "A2" length.
In Group B, the same measurements of working length and patency controls were performed, but the simulated lateral canals were prepared at 6 mm from the end of the root. The size 15 engine reamer measurements were recorded as the "B1" lengths, and the size 20 enlarged measurements were recorded as the "B2" lengths.
Statistical Analyses
The data were analyzed by one-way analysis of variance. Within each group, the control measurements (true working lengths as determined by the electronic apex locator) were compared with the measurements of working length obtained after creation of the lateral canals (A1 and A2 lengths for group A, with lateral canals at 3 mm; B1 and B2 lengths for group B, with lateral canals at 6 mm).
Results
In Group A (simulated lateral canals at 3 mm), there were no significant differences between the true working length and the A1 and A2 measurements, all measured by the electronic apex locator (p > 0.05) (Fig. 2).
 Figure 2: Working length of samples in group A (mean of 3 determinations), for simulated lateral canals at 3 mm. True working length is the working length determined by the electronic apex locator before preparation of simulated lateral canals.
Figure 2: Working length of samples in group A (mean of 3 determinations), for simulated lateral canals at 3 mm. True working length is the working length determined by the electronic apex locator before preparation of simulated lateral canals.
In Group B (simulated lateral canals at 6 mm), there were no significant differences between the true working length and the B1 and B2 measurements, all measured by the electronic apex locator (p > 0.05) (Fig. 3).
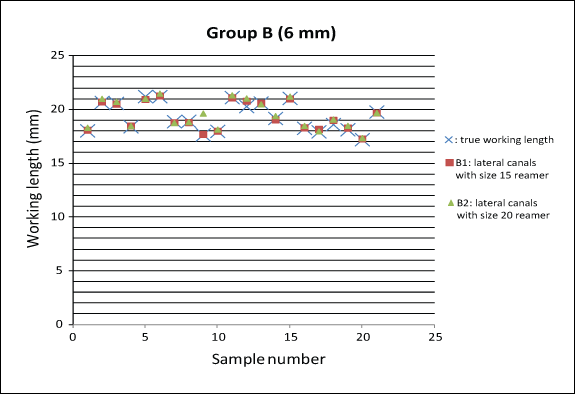 Figure 3: Working length of samples in group B (mean of 3 determinations), for simulated lateral canals at 6 mm. True working length is the working length determined by the electronic apex locator before preparation of simulated lateral canals.
Figure 3: Working length of samples in group B (mean of 3 determinations), for simulated lateral canals at 6 mm. True working length is the working length determined by the electronic apex locator before preparation of simulated lateral canals.
Discussion
This study was undertaken to evaluate the in vitro accuracy and predictability of the Justy II electronic apex locator for determining working length in roots with different-sized simulated lateral canals at different levels. This device uses the ratio method introduced by Kobayashi and Suda,9 which is based on calculation of the quotient of 2 simultaneously measured impedances of 2 different frequencies to reveal the position of the endodontic file tip in the root canal. Like most modern electronic apex locators, the Justy II device is also capable of recording the point at which the tissues of the periodontal ligament begin outside the canal. Thus, the device marks as the apex the first point where there is periodontal communication. These areas of communication may indeed represent the real apex, but they could also be horizontal or vertical fractures, perforations or lateral canals. In a previous study, Topuz and colleagues7 reported that 2 ratio-method electronic apex locators with integrated endodontic motors both detected simulated horizontal and vertical root fractures (periodontal communication areas) as the apex within an acceptable range. In addition, Azabal and colleagues3 reported that the Justy II apex locator accurately determined the position of simulated horizontal and vertical root fractures.
In previous studies, 61.3% of lateral branches in mandibular incisors10 and 70.1% of lateral branches in maxillary central incisors had a thickness less than that of a size 10 reamer.11 In the current study, lateral branches of greater diameter (reamer sizes 15 and 20) were prepared, on the assumption that larger lateral canals would have greater effects on the electronic apex locator.
For maintenance of electrical conductivity, previous studies have used various media.12,13 Given the relatively small diameter of the simulated lateral canals and the necessity of fluidity of the medium, to ensure the presence of an electric circuit in the root canal, saline solution was used as the medium in this study, as proposed by Ushiyama.14
In previous studies, the determination of working length was influenced by the size of the canal at the apical terminus.15-17 In the study reported here, there was no attempt to standardize the size of the apical terminus of the specimens. Instead, specimens with mature apices were selected, and all roots were prepared with master apical files of the same size.
For both groups, 2.25% NaOCl was used as the irrigation solution, because it was desirable to simulate clinical conditions; use of this solution was feasible because electronic apex locators that use the ratio method are not affected by the contents of the root canal.18
From previous studies, it was known that precise determination of the position of the file tip can be achieved only by histological examination under a microscope,19 but this approach is not feasible in the clinical setting. Earlier observations indicated that when a file tip is placed 1 mm short of the anatomic apex, it will be within a range at which the apical construction is generally located.20,21 In addition, Jung and colleagues22 evaluated the reliability of the "0.5" and "APEX" mark measurements of 2 electronic apex locators. For both devices, the authors reported no significant difference in the reliability of these 2 marks for locating the major foramen. They concluded that knowing what each mark indicates is more relevant for determining the working length than selecting a particular mark. In the current study, efforts were made to detect a point between the apical construction and the major foramen as a target interval. Therefore, 0.5 mm was subtracted from the total length of each tooth to determine the true working length for the purposes of tooth preparation. In addition, the Justy II device was used with 0.5-mm accuracy to the apex to simulate clinical conditions. However, the visually determined true working length was not compared with true working length as determined by the electronic apex locators. Instead, for more reliable results, the working lengths determined by the electronic apex locator, all measured at 0.5-mm accuracy, were compared within each group of teeth. Comparing the visually determined true working length with working length as determined by an electronic apex locator should be the subject of a future study.
Although a few studies have examined the behaviour of apex locators in cases of root fracture and perforation,3,4,7 the behaviour and accuracy of a ratio-based electronic apex locator for roots with simulated lateral canals have not previously been evaluated. It was therefore impossible to compare the results of this study with those of similar studies.
In this in vitro study, the accuracy of the ratiobased Justy II electronic apex locator was evaluated for roots with simulated lateral canals of 2 different sizes at 2 different levels. The accuracy of this brand of locator was not affected by the presence or location of the simulated lateral canals, and the device was able to determine the apex with acceptable accuracy.
THE AUTHORS
|
Dr. Uzun is associate professor, restorative treatment and endodontics, Gazi University, faculty of dentistry, Ankara, Turkey. |
|
|
Dr. Topuz is associate professor, restorative treatment and endodontics, Gazi University, faculty of dentistry, Ankara, Turkey. |
|
|
Dr. Aslan is assistant researcher, restorative treatment and endodontics, Gazi University, faculty of dentistry, Ankara, Turkey. |
|
|
Dr. Tınaz is professor, restorative treatment and endodontics, Gazi University, faculty of dentistry, Ankara, Turkey. |
Corresponding Author: Dr. Özgür Uzun, Gazi University, Faculty of dentistry, Department of operative dentistry and endodontics, 82.St. Emek, 06510 Ankara, Turkey.
Email: drdtozguruzun@yahoo.com
References
- American Association of Endodontists Glossary of endodontic terms. 2003; 7th edition. Available: http://dev.aae.org/glossary/ (accessed 2012 May 14)
- Nekoofar H, Ghandi MM, Hayes SJ, Dummer PM. The fundamental operating principles of electronic root canal length measurement devices. Int Endod J. 2006;39(8):595-609.
- Azabal M, Garcia-Otero D, Macorra JC. Accuracy of the Justy II Apex Locator in determining working length in simulated horizontal and vertical fractures. Int Endod J. 2004;37(3):174-7.
- Ebrahim AK, Wadachi R, Suda H. Accuracy of three different electronic apex locators in detecting simulated horizontal and vertical root fractures. Aust Endod J. 2006;32(2):64-9.
- Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endodontic Topics. 2005;10:3-29.
- De Deus QD. Frequency, location and direction of the lateral, secondary and accessory canals. J Endod. 1975;1(11):361-6.
- Topuz O, Uzun O, Tinaz AC, Bodrumlu E, Görgül G. Accuracy of two apex-locating handpieces in detecting simulated vertical and horizontal root fractures. J Endod. 2008;34(3):310-3.
- Thomas AS, Hartwell GR, Moon PC. The accuracy of the Root ZX electronic apex locator using stainless-steel and the nickel-titanium files. J Endod. 2003;29(10):662-3.
- Kobayashi C, Suda H. New electronic canal measuring device based on the ratio method. J Endod. 1994;20(3):111-4.
- Miyashita M, Kasahara E, Yasuda E, Yamamoto A, Sekizawa T. Root canal system of the mandibular incisor. J Endod. 1997;23(8):479-84.
- Kasahara E, Yasuda E, Yamamoto A, Anzai M, et al. Root canal system of the maxillary central incisor. J Endod. 1990;16(4):158-61.
- Kaufman AY, Katz A. Reliability of Root ZX apex locator tested by an in vitro model. J Endod. 1993;19:201 (abstract).
- Tinaz AC, Alacam T, Topuz O. A simple model to demonstrate the apex locator. Int Endod J. 2002;35:940-5.
- Ushiyama J. New principle and method for measuring the root canal length. J Endod. 1983; 9(3):97-104.
- Fan W, Fan B, Gutmann JL, Bian Z, Fan MW. Evaluation of the accuracy of three electronic apex locators using glass tubules. Int Endod J. 2006;39(2):127-35.
- Saito T, Yamashita Y. Electronic determination of root canal length by newly developed measuring device: influences of the diameter of apical foramen, the size of K file and the root canal irrigants. Dent Jpn (Tokyo). 1990;27(1):65-72.
- Nguyen HQ, Kaufman AY, Komorowski RC, Friedman S. Electronic length measurement using small and large files in enlarged canals. Int Endod J. 1996;29(6):359-64.
- Christie WH, Peikoff MD, Hawrisch CE. Clinical observations on a newly designed electronic apex locator. J Can Dent Assoc. 1993;59(9):765-72.
- Hoer D, Attin T. The accuracy of electronic working length determination. Int Endod J. 2004;37(2):125-31.
- Kuttler Y. Microscopic investigation of root apexes. J Am Dent Assoc. 1955;50(5):544-62.
- Nahmias Y, Aurelio JA, Gerstein H. Expanded use of the electronic canal length measuring devices. J Endod. 1983;9(8):347-9.
- Jung IY, Yoon BH, Lee SJ, Lee SJ. Comparison of the reliability of “0.5” and “APEX” mark measurements in two frequency-based electronic apex locators. J Endod. 2011;37(1):49-52.