
Abstract
Introduction: The Canadian Dental Association recommends that children have their first visit to a dental professional no later than 12 months of age. In 2010, the Manitoba Dental Association launched the Free First Visit (FFV) program to increase access to early visits in the province. The purpose of the study reported here was to survey dentists about their views on the FFV program and to gain an understanding of their attitudes and practice patterns relating to the oral health of infants and toddlers and first dental visits.
Methods: A survey was mailed to registered general and pediatric dentists in Manitoba according to a modified Dillman methodology. Dentists were asked about their views on the FFV, their knowledge of early childhood oral health and the timing of first dental visits. Descriptive statistics, bivariate analyses and logistic regression analyses were performed. A p value of 0.05 or less was considered significant.
Results: The overall response rate was 63.2% (375 eligible responses out of 593 surveys mailed). The majority of respondents were men (255/373 [68.4%]), and most respondents were general dentists (355/372 [95.4%]). A total of 63.5% (231/364) felt that the FFV program improved access to care, 64.6% (223/345) believed that public awareness of young children’s oral health has increased, and 76.2% (266/349) thought that the FFV initiative should continue past the planned end date of March 31, 2013. On average (± standard deviation), respondents thought that the first dental visit should occur at 18.1 ± 10.0 months, but in their practices, they actually recommended a slightly older age (18.9 ± 10.4 months). Compared with results from a previous survey, conducted in 2005, dentists who responded to this survey recommended that children have their first visit at a significantly younger age. A greater proportion of dentists reported seeing children 12–23 months of age in their practices than in the past (81.9% vs. 73.7%).
Conclusions: A majority of dentists who responded to the survey approved of the FFV program and thought it should continue. Although these dentists recommended early first dental visits, the average age recommended by respondents was 6 months later than the target age of 12 months. It appears that, over time, dentists are becoming more aware of prevention and management techniques relating to infants and toddlers.
Early dental care is an important strategy to reduce the incidence of early childhood caries (ECC). The prevalence of caries among preschool-aged children appears to be increasing.1 Severe forms can adversely affect overall health and quality of life.2 Provincial dental surgery statistics indicate that many children are not benefiting from proactive early dental care.3,4 Keeping children cavity-free can have lifelong benefits, as those with caries at an early age are more likely to experience future dental problems.5-7 Conversely, good oral health care during early life sets the foundation for a lifetime of good dental health. The Canadian Dental Association (CDA), the Canadian Academy of Pediatric Dentistry and the American Academy of Pediatric Dentistry recommend a first dental visit corresponding with eruption of the first primary tooth and no later than 12 months of age.8-10 The rationale for this recommendation is that it establishes a long-term “dental home” for the child,11 an important step in ensuring that children remain caries-free.12 However, such guidelines only inform behaviour; they do not necessarily lead to behaviour change. Past oral health promotion activities in Manitoba showed that few dental professionals were willing to provide early visits. Concern about this situation prompted a 2005 survey of Manitoba dentists, which identified a lack of awareness of the recommendation on timing of the first dental visit.13 At that time, many dentists were not seeing very young children, with only half reporting that they saw children by the recommended milestone.13 The Manitoba Dental Association (MDA) was made aware of these concerns and reviewed the results of the earlier survey. The association determined that a program was needed to promote early dental visits in the province.
Therefore, on April 1, 2010, the MDA launched its Free First Visit (FFV) program, to provide access to no-cost dental screenings for children up to 36 months of age. Participating dentists were asked to provide these visits pro bono. The program was implemented as a 3-year campaign. The MDA developed promotional and educational resources to educate the public and provided dentists with regular updates to prepare and equip them to see young children. These updates included tips on how to examine infants and toddlers, a review of the factors that contribute to ECC, suggestions about anticipatory guidance to provide to parents and caregivers, and information to help practitioners to overcome their reservations about caring for young children. During an FFV, the dentist assesses the child’s oral health and risk of caries. The dentist then recommends further care if appropriate and educates parents on their role in maintaining good oral health for their child.
The purpose of the current study was to survey dentists about their views on the FFV program and to develop an understanding of their attitudes and practice patterns relating to oral health and first visits among infants and toddlers.
Methods
Approval for the study was granted by the Health Research Ethics Board, University of Manitoba, and by the MDA. The study population consisted of general and pediatric dentists practising in the province of Manitoba, Canada, during 2011. The sampling frame was the MDA membership registry. The survey was designed to determine what dentists thought of the FFV program and whether their awareness of the need for early visits and their knowledge, attitudes and practice behaviours relating to dental care for young children had improved since the previous survey. The tool was a modified version of the one used in 200x to determine Manitoba dentists’ awareness of early childhood oral health and early visits.13 The author team worked with the MDA to adapt this instrument for the needs of the current evaluation project. The survey consisted of questions about the FFV program, respondents’ views and knowledge of early childhood oral health and first visits, and respondents’ demographic characteristics.
A modified Dillman survey methodology was followed to improve the response rate.14 In November 2011, a cover letter, survey and stamped return envelope were mailed to potential participants. Two weeks later, a reminder letter was sent to all participants. In December 2011, one month after the initial mailing, a second package was sent to nonrespondents, with another reminder letter 2 weeks later. In mid-January 2012, a third full mailing was sent to nonrespondents, and a final mailing occurred in February 2012. Data were entered into an Excel database (Microsoft Office 2003) and analyzed using NCSS software (Kaysville, UT). Statistical analyses included calculation of descriptive statistics (frequencies, means and standard deviations [SDs]). Bivariate analyses involved chi-square analysis, t tests and analysis of variance. Logistic regression analysis was also performed to determine variables associated with recommending a first visit by 12 months of age. A p value of 0.05 or less was considered significant. Results from the previous survey were used as baseline measures of dentists’ awareness of infant oral health and ECC, to gauge changes over time.
Results
A total of 593 surveys were mailed to registered general and pediatric dentists. Overall, 398 surveys were returned, of which 23 were excluded because the dentist had moved, was no longer in practice or refused to participate. The final sample consisted of 375 dentists (217 [57.9%] who responded to the November 2011 mailing, 93 [24.8%] to the December 2011 mailing, 27 [7.2%] to the January 2012 mailing and 38 [10.1%] to the February 2012 mailing), for an overall response rate of 63.2% [375/593].
Description of Participants
The majority of respondents were men (255/373 [68.4%]), and most were general practitioners (355/372 [95.4%]) (Table 1). The average age was 45.7 ± 12.3 years, and the median year of graduation was 1990. Infants (1–23 months) and preschoolers (24–71 months) accounted for only 2.7% ± 4.4 % and 6.8% ± 8.9 % of respondents’ practices.
Views of the FFV Program
Essentially all respondents (370/373 [99.2%]) were aware of the MDA’s FFV program, with nearly 2 out of every 3 (235/364 [64.6%]) being registered in the program. The majority (231/365 [63.3%]) agreed that the program improved access to care for young children (Table 2).
NOTE: Click to enlarge Tables.
Table 1 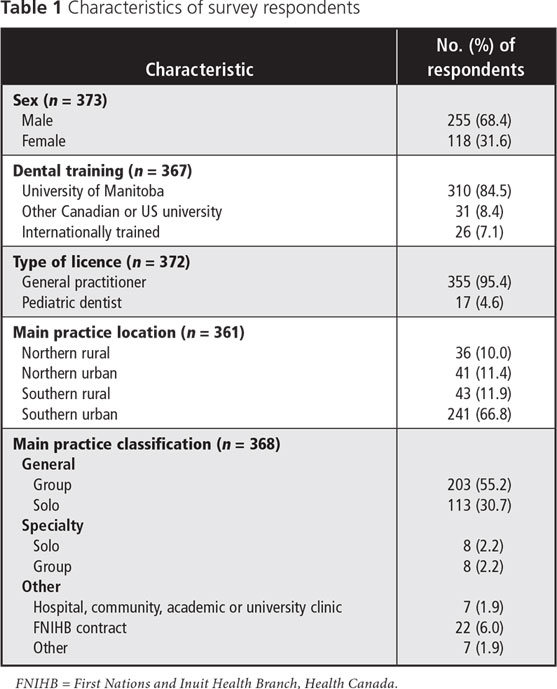
Table 2 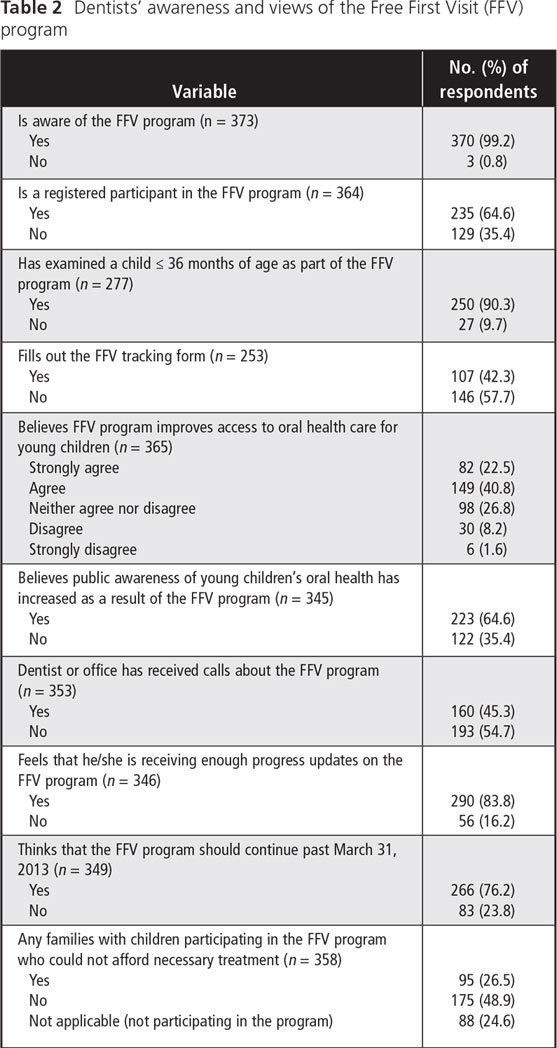
A total of 90.3% of respondents (250/277) indicated that they had already examined a child up to 36 months of age as part of the FFV initiative. The mean number of children seen under the program, as reported by respondents, was 25.0 ± 53.0 (median 10.0). However, only 42.3% (107/253) reported routinely completing the tracking form for the FFV program, which the MDA implemented for evaluation purposes.
Overall, 64.6% (223/345) believed that public awareness of young children’s oral health had increased as a result of the program, and 76.2% (266/349) thought the initiative should continue past its original end date of March 31, 2013.
Among those not participating in the program (n = 129), key reasons for not participating included “few parents requesting FFVs” (55/95 [57.9%]), “uncomfortable seeing uncooperative children” (31/95 [32.6%]), “too much paperwork to complete the tracking forms” (28/89 [31.5%]), “uncomfortable seeing crying children” (28/93 [30.1%]) and “too busy” (23/91 [25.3%]) (Table 3).
Views on Early Childhood Oral Health and Timing of First Dental Visits
Responses to questions about the timing of early visits and early childhood oral health (Table 4) were contrasted with responses to the same questions in the previous survey of Manitoba-based dentists.13 Participants in the 2 surveys were well matched with respect to the type of licence (p = 0.40) and sex ratio (p = 0.16).
When asked what age they thought children should have their first dental visit, respondents to the current survey indicated 18.1 ± 10.0 months (range 1–60 months). However, the average age actually recommended, as reported by these same respondents, was 18.9 ± 10.4 months (range 1–60 months). Paired t tests revealed that, in practice, dentists recommended a significantly older age for the first visit than what they thought should be the age of the first visit (p = 0.002). Relative to the previous survey, there were significant improvements in these 2 measures in the current survey, with respondents thinking and recommending that children should have their first dental visit at a significantly younger age (Table 4).
Table 3 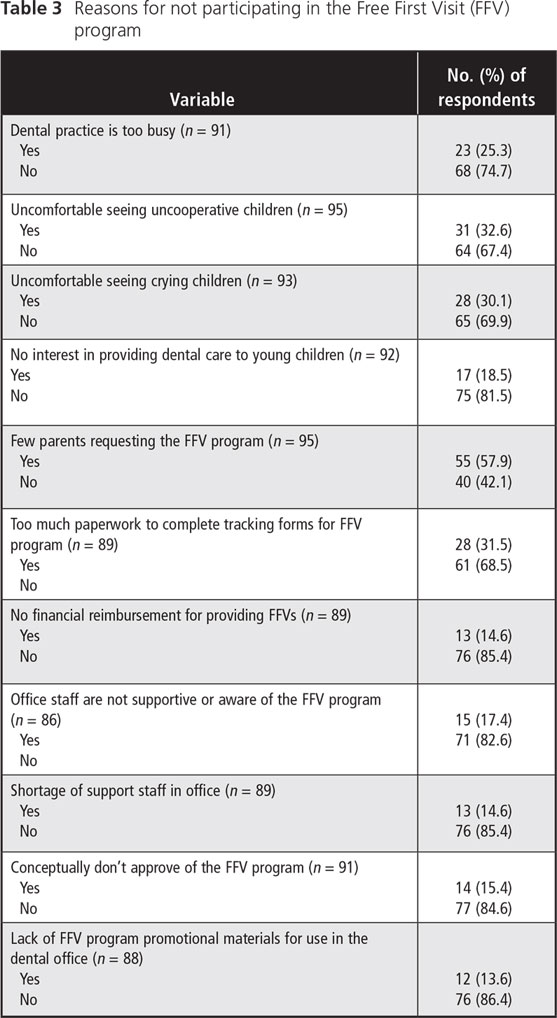
Table 4 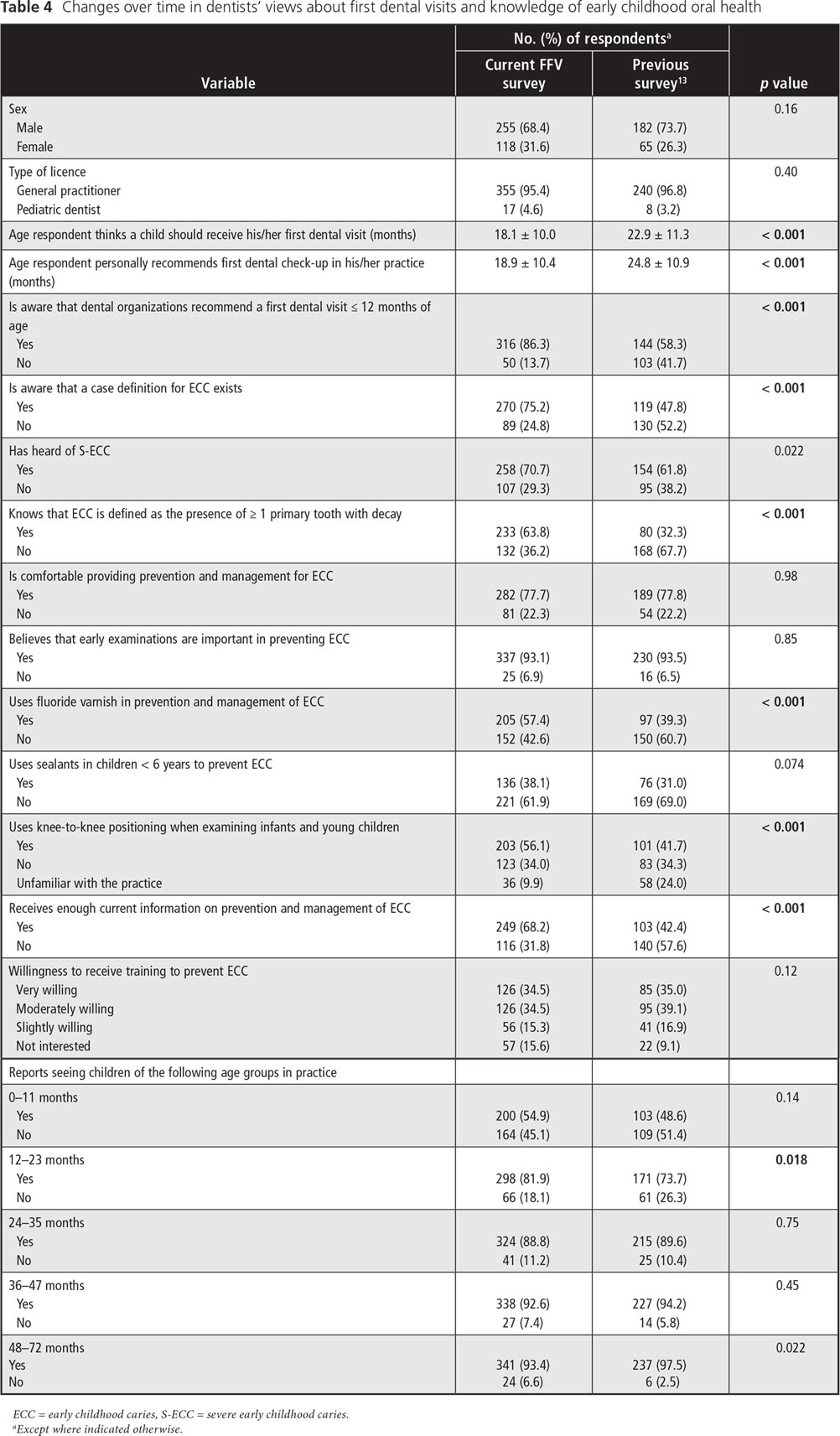
There was improvement in most parameters surveyed when compared to the responses to the same questions posed in the previous survey, but not all were significant (Table 4). In terms of knowledge of early oral care, there was significant improvement in awareness of professional organizations’ recommendations for a first visit (p < 0.001), awareness that a case definition for ECC exists (p < 0.001) and awareness of how ECC is defined (p < 0.001).
Respondents appeared to be comfortable providing prevention and management for ECC (282/363 [77.7%]) and believed that early examinations are important in preventing ECC (337/362 [93.1%]), but these proportions had not changed significantly since the previous survey (p = 0.98 and p = 0.85, respectively) (Table 4). Relative to the previous survey, a significantly greater proportion of dentists reported seeing children 12–23 months of age in their practices (p < 0.018). Although comfort level in caring for young children did not change over time, far more dentists reported using knee-to-knee positioning techniques for examinations and applying fluoride varnish.
Differences in the recommended age for a first visit were analyzed by reviewing responses to certain questions posed in the survey (Table 5). Those in favour of continuation of the FFV program were more likely to recommend earlier first visits than those who did not favour continuation (p < 0.001). Similarly, the mean recommended age for a first visit was significantly younger among those who were aware of professional recommendations regarding a first dental visit (p < 0.001). Those who believed that early examinations are important in preventing ECC also recommended earlier visits (p < 0.001). The recommended age for a first visit was significantly younger among female respondents than among their male counterparts (p < 0.001) and among pediatric dentists relative to general dentists (p < 0.001).
Regression Analysis
Variables independently associated with recommending a first visit at or below 12 months of age, identified by logistic regression analysis, included age of the dentist, type of licence and belief that the FFV program should continue (Table 6). Specifically, younger dentists and pediatric dentists recommended a first visit at a younger age.
Table 5 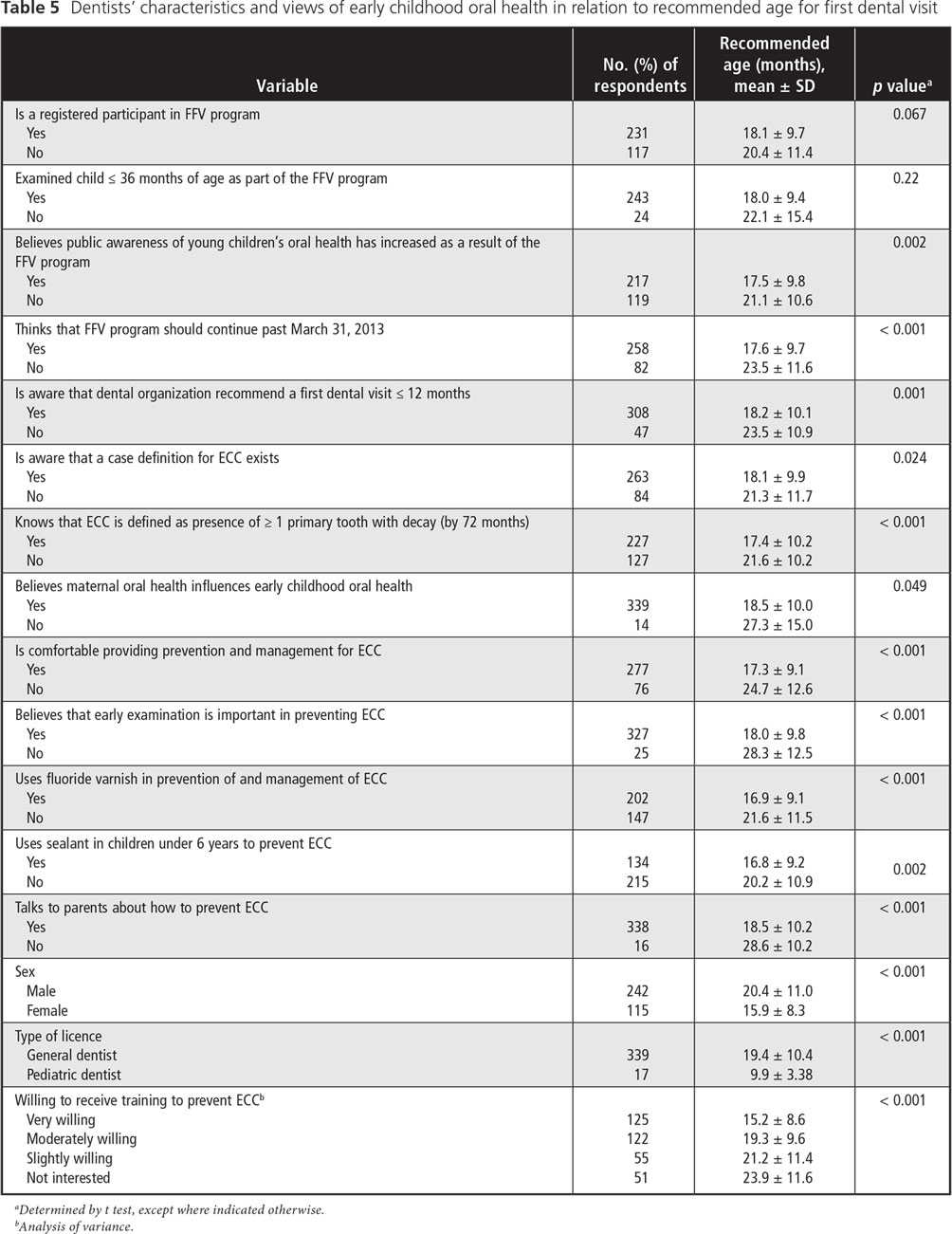
Table 6 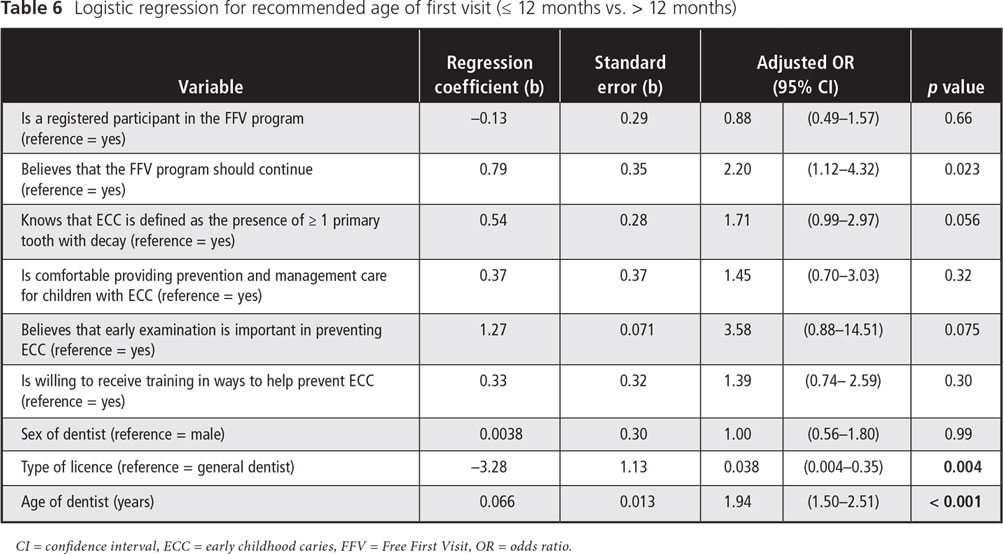
Discussion
This study explored dentists’ views on a province-wide program promoting early dental visits, with the goal of understanding their knowledge and practice habits related to the oral health of infants and toddlers. Most respondents to the survey were in favour of the program and thought it should continue beyond the planned end date of March 31, 2013.
Before the program began, the MDA developed a strategy to inform members about the concept of first visits and the FFV program. This communications strategy was started more than 1 year in advance of program initiation. The MDA sent invitation letters to dentists describing the program and published a series of articles in the association’s newsletter on the importance of infant oral health, the risk factors for ECC, methods of examining an infant or toddler, and methods of determining the risk of caries. The public campaign included press releases and a kick-off at the association’s annual convention in January 2010, media spots and advertisements on the back of public transit buses.
According to data collected in the survey reported here, the most important barrier to participation was that few parents were requesting the FFV for their children. This result is intriguing, considering that the MDA spent considerable resources to promote the program and given that most respondents to the survey believed that the program had improved public awareness of infant and toddler oral health. Other notable barriers involved providers’ aversion to caring for uncooperative and crying children, barriers that were also identified by other researchers.13,15 This aversion may be due to limited clinical experience with infant and toddler oral health during training and little continuing education on the topic. However, all dentists have a professional responsibility to promote the concept of early first dental visits.10,13
Fortunately, the proportion of dentists seeing 1-year-old children has improved significantly over the past few years, and the findings presented here are more favourable than those of 2 recent US surveys, which reported that fewer than half of general dentists routinely cared for infants and toddlers.16,17 In fact, there has been a remarkable shift since the 2005 survey, with Manitoba dentists recommending a first visit around 19 months of age. Although this is slightly more than 6 months older than current recommendations from the CDA and other organizations, it is a statistically significant reduction of nearly 6 months since the earlier survey.13 This likely means that there is greater access for young children today than there was over 6 years ago. It may take another decade before the concept of first visits no later than 12 months of age is entrenched in practice. However, it is not known whether dentists’ recommendations, as indicated by responses in the survey, match what they do in practice. The degree to which the FFV program has helped to inform dentists and to promote these changes in practice is unknown, but it is likely considerable. Other reasons for the shift in practice may be the reaffirmation of the CDA’s position on ECC and early visits, the efforts of the “Healthy Smile, Happy Child” initiative in Manitoba and an increase in demand from parents.10,18 Whatever has contributed to these improvements, caution is warranted in interpreting these survey results, as this survey is only one aspect of the mixed-methods evaluation of the FFV program. Another activity involves tracking the number of children seen (by means of tracking forms completed in dental offices) and using geo-mapping software to map visits on the basis of postal codes. If the estimates of respondents to the current survey are correct, then we estimate that 5,618 children benefited from an FFV during the first 20 months of the program. Focus groups have also been held with dentists and parents of young children. Collectively, this information will assist and inform the MDA in determining whether the FFV program should be continued and if so, how it could be enhanced. In fact, while the 3-year trial of the FFV program ended March 31, 2013, the MDA is still promoting the FFV program and participating dentists have been asked to continue providing this service.
Various strategies can be used to increase provider and public knowledge and awareness of pediatric oral health and first dental visits, including professional education, articles in journals and magazines, and advertising. Community-based workshops have improved knowledge among non-dental service providers (e.g., health care personnel and early childhood educators) and community members about the importance of the 12-month visits, when to start brushing, when to wean children from the bottle and the transmissibility of cariogenic bacteria.18
Somewhat surprising was the fact that, in contrast to the initial hypothesis, those not participating in the FFV program were not more apt to recommend an older age for a first visit. However, those who felt that the FFV program should continue beyond the original 3- year mandate were more likely to recommend earlier visits. Other findings were similar to those of the previous survey,13 as female dentists, pediatric specialists and those willing to receive additional training in ECC prevention recommended significantly earlier first visits.
Younger dentists were significantly more likely to recommend first visits by the 12-month milestone. Recent graduates are more likely to have been taught these recommendations in the undergraduate curriculum.13 However, there is a need to survey dental faculties to determine what is being taught about infant and toddler oral health and what training methods are being employed, including whether students receive hands-on training on performing infant dental examinations.
The challenge for dental leaders and researchers is how to effectively inform dentists of recommendations for early visits and any new guidelines that may arise in the future. Practice change is not easy and may take time. The results of the current study suggest that dentists’ familiarity with ECC and its prevention have improved over time, with greater awareness of how ECC is defined, the benefits of fluoride varnish and the positioning techniques that facilitate early dental examinations. Making dentists more comfortable in caring for this population will undoubtedly help. However, the profession may need to look to innovative knowledge transfer techniques to align clinical practice behaviours with current policies and recommendations.13 Another consideration warranting attention is how to ensure that children at moderate to high risk for caries, such as First Nations and economically disadvantaged children, benefit from early visits.1,19,20
Public health campaigns developed by health professionals to encourage healthy lifestyles, such as the FFV program, may have limited impact in terms of promoting health.21 Nonetheless, although it may not be the most effective route for improving dental health, the FFV program is improving the awareness of dentists and the public at large, thereby leading to greater adoption of early dental visits.Other helpful strategies are those that involve changing health and social policy and those that make healthy choices more affordable and convenient.21The MDA’s FFV program could be considered one such policy change.
Survey-based research like that reported here has certain limitations, such as those related to response rate. Fortunately, the response rate in the current study was relatively good and was similar to the baseline survey,13 possibly because of repeated attempts to contact nonrespondents. Another concern is whether the wording of some questions and their sequencing in the survey might have introduced bias. To minimize any influence of question sequencing, the order of questions used in the current survey was kept the same as that in the baseline questionnaire. Another potential limitation is recall bias, as respondents were required to estimate their practice habits and behaviours, and response bias, whereby dentists may have responded in a specific way to appear more knowledgeable. Finally, those responding to this survey may have been biased and more likely to be concerned about pediatric oral health issues and supportive of the FFV program than were nonrespondents.
THE AUTHORS
 |
Dr. Schroth is assistant professor, department of preventive dental science, faculty of dentistry, and department of pediatrics and child health, faculty of medicine, University of Manitoba; and research scientist, Manitoba Institute of Child Health. |
 |
Mr. Yaffe is a student, faculty of nursing, University of Manitoba; and research assistant, Manitoba Institute of Child Health. |
 |
Ms. Edwards is regional director, primary health care and chronic disease, Winnipeg Regional Health Authority; and special advisor to the deputy minister of health on primary care, Manitoba Health. |
 |
Dr. Hai-Santiago is provincial oral health consultant, Manitoba Health. |
 |
Ms. Ellis is executive director, clinical services, Northern Health Authority. |
 |
Dr. Moffatt is professor, department of community health sciences and department of pediatrics and child health, faculty of medicine, University of Manitoba; research scientist, Manitoba Institute of Child Health; and executive director of research and applied learning, Winnipeg Regional Health Authority. |
 |
Manitoba Dental Association (www.manitobadentist.ca) |
Acknowledgements: This research was made possible through an operating grant from the Manitoba Institute of Child Health. Dr. Schroth holds a Manitoba Medical Service Foundation/Manitoba Health Research Council Clinical Research Professorship in Population Medicine. Aaron Yaffe received a summer studentship from the Manitoba Institute of Child Health. The team would also like to recognize the support of the Manitoba Dental Association’s Free First Visit Committee (Drs. Charles Lekic, Lanny Jacobs, Robert Schroth, Leon Stein, and Linda Berg) and members of the “Healthy Smile, Happy Child” partnership. Thank you to Betty-Anne Mittermuller for her assistance with data entry.
Correspondence to: Dr. Robert J Schroth, University of Manitoba, 507–715 McDermot Ave., Winnipeg, MB R3E 3P4. Email: umschrot@cc.umanitoba.ca.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- Dye BA, Tan S, Smith V, Lewis BG, Barker LK, Thornton-Evans G, et al. Trends in oral health status: United States, 1988-1994 and 1999-2004. Vital Health Stat 11. 2007;(248):1-92.
- Schroth RJ, Harrison RL, Moffatt ME. Oral health of indigenous children and the influence of early childhood caries on childhood health and well-being. Pediatr Clin North Am. 2009;56(6):1481-99.
- Schroth RJ, Morey B. Providing timely dental treatment for young children under general anesthesia in a government priority. J Can Dent Assoc. 2007;73(3):241-3.
- Brownell M, DeCoster C, Penfold R, Derksen S, Au W, Schultz J, et al. Manitoba Child Health Atlas Update. Winnipeg, MB: Manitoba Centre for Health Policy; 2008: 1-318.
- al-Shalan TA, Erickson PR, Hardie NA. Primary incisor decay before age 4 as a risk factor for future dental caries. Pediatr Dent. 1997;19(1):37-41.
- Li Y, Wang W. Predicting caries in permanent teeth from caries in primary teeth: an eight-year cohort study. J Dent Res. 2002;81(8):561-6.
- Peretz B, Ram D, Azo E, Efrat Y. Preschool caries as an indicator of future caries: a longitudinal study. Pediatr Dent. 2003;25(2):114-8.
- American Academy of Pediatric Dentistry. Early childhood caries (ECC): classifications, consequences, and preventive strategies. Pediatr Dent. 2012;34(6):50-2.
- Canadian Dental Association. Ottawa. CDA position on first visit to the dentist. Canadian Dental Association [Approved 2005; reaffirmed 2012; accessed 2013 Aug 13]. Available: http://www.cda-adc.ca/en/about/media_room/position_statements/
- Canadian Dental Association. Ottawa. CDA Position on Early Childhood Caries. Canadian Dental Association [approved 2010 Apr; accessed 2013 Aug 13]. Available: http://www.cda-adc.ca/en/about/media_room/position_statements/
- American Academy of Pediatric Dentistry. Policy on the dental home. Pediatr Dent. 2012;34(6):24-5.
- Melhado FL, Cunha RF, Nery RS. Influence of dental care for infants on caries prevalence: a comparative study. J Dent Child (Chic). 2003;70(2):120-3.
- Stijacic T, Schroth RJ, Lawrence HP. Are Manitoba dentists aware of the recommendation for a first visit to the dentist by age 1 year? J Can Dent Assoc. 2008;74(10):903.
- Dillman D. Mail and internet surveys: the tailored design method. 2nd ed. New York: Wiley; 1999.
- Hussein AS, Schroth RJ, Abu-Hassan MI. General Dental Practitioners' Views on Early Childhood Caries and Timing of the First Dental Visit in Selangor, Malaysia. Asia Pac J Public Health. 2013 Feb 17. [Epub ahead of print]
- Brickhouse TH, Unkel JH, Kancitis I, Best AM, Davis RD. Infant oral health care: a survey of general dentists, pediatric dentists, and pediatricians in Virginia. Oral Health. 2010;100(1):22-4, 27-8, 30.
- Garg S, Rubin T, Jasek J, Weinstein J, Helburn L, Kaye K. How willing are dentists to treat young children?: a survey of dentists affiliated with Medicaid managed care in New York City, 2010. J Am Dent Assoc. 2013;144(4):416-25.
- Macintosh AC, Schroth RJ, Edwards J, Harms L, Mellon B, Moffatt M. The impact of community workshops on improving early childhood oral health knowledge. Pediatr Dent. 2010;32(2):110-7.
- Irvine J, Holve S, Krol D, Schroth R. Early childhood caries in indigenous communities. A joint statement with the American Academy of Pediatrics. Paediatr Child Health. 2011;16(6):351-64.
- American Academy of Pediatrics, Committee on Native American Child Health, Canadian Paediatric Society, First Nations, Inuit and Métis Committee. Early childhood caries in indigenous communities. Pediatrics. 2011;127(6):1190-8.
- Kreindler SA. Lifting the burden of chronic disease: what has worked? What hasn't? What's next? Healthc Q. 2009;12(2):30-40.