Various obturation techniques have been proposed for the 3-dimensional filling of root canals,1-3 with thermoplasticized materials showing the most promising results.4,5 Minimizing voids can avert apical and coronal microinfiltration by microorganisms and their byproducts,6,7 thereby preventing persistent or secondary infection leading to endodontic treatment failure.8,9 Whenever possible, the first choice in cases of treatment failure should be nonsurgical endodontic retreatment. The complexity of this procedure is directly related to the material originally used to fill the root canal.10
A specific obturation technique uses a carrier covered by gutta-percha, which is heated in a special oven. Warming allows the gutta-percha to flow and fill the root canal system. The carrier remains enveloped in the filling mass. In 1978, Johnson11 proposed the use of a metal carrier and this was later marketed as the Thermafil system (Dentsply Tulsa Dental Specialties, Tulsa, Okla., USA). Metal carriers were later replaced with plastic, the latter being easier and faster to remove in the event of retreatment or post-space preparation.12 More recently, a third-generation carrier called GuttaCore (Dentsply Tulsa Dental Specialties) was developed; it consists of cross-linked gutta-percha instead of plastic. According to the manufacturer, this system is easier to remove and is sufficiently rigid to guide the gutta-percha into the root canal.13
The ideal filling material should be readily removable from the root canal when necessary.14 Consequently, potential new filling materials should be assessed for ease and efficiency of removal. To date, no study has compared these techniques with regard to residual filling material after root canal retreatment. Therefore, the aim of this ex vivo study was to compare the amount of residual filling material and removal times in retreated root canals filled with GuttaCore and Thermafil carriers.
Materials and Methods
The protocol followed in this study was carried out by a single operator after approval by the Research Ethics Committee of the University of Pernambuco (Camaragibe, PE, Brazil; protocol CAAE 03868512.5.00005207) and was performed in accordance with the terms of the Declaration of Helsinki.15
Sample Selection and Preparation
Using radiographic examination, maxillary central incisors with an intact pulp chamber and a straight single canal were included in this study; teeth with internal or external root resorption, incomplete root development, pulp calcification or a canal with a curvature of over 20° were excluded. Forty-five maxillary incisors were selected and stored in a 0.1% thymol solution until use.
Crowns were removed using a diamond disc (Axis SybronEndo, Coppell, Tex., USA) to produce a standard root size of 18 mm as measured with callipers. A #15 K-type file (Dentsply Tulsa Dental Specialties) was introduced into the canal until visible at the apical foramen under a dental operating microscope (OPMI Pico, Zeiss, Göttingen, Germany) at 5× magnification. The working length was set at 1 mm short of the apical foramen.
Canal Instrumentation
Cervical and middle thirds of each canal were preflared with Gates-Glidden drills numbers 4, 3 and 2 (Dentsply Tulsa Dental Specialties), and the root canal was instrumented up to an F4 Protaper Universal rotary file (Dentsply Tulsa Dental Specialties), according to the manufacturer's instructions. Apical preparation was completed with a #40 K-type hand file (Dentsply Tulsa Dental Specialties). Canals were irrigated with 5 mL of 6% sodium hypochlorite at every instrument change using a syringe and an open-end 30G needle (NaviTip, Ultradent Products, South Jordan, Utah, USA) positioned 2 mm short of the working length in a back-and-forth motion. Cleaning after instrumentation consisted of irrigation with 5 mL of 17% EDTA, agitation for 1 minute with the aid of a sonic device (EndoActivator, Dentsply Tulsa Dental Specialties), followed by application of 5 mL of 6% sodium hypochlorite. Canals were dried using paper points.
Obturation Techniques
The teeth were randomly divided into 3 groups of 15 specimens each (n=15). The same resin-based sealer (ThermaSeal Plus Ribbon, Dentsply Tulsa Dental Specialties) was used in all groups and mixed according to the manufacturer's directions. The same amount of sealer (5-mm) was applied to each sample with the aid of absorbent paper points.
Thermafil Group: Before drying the canal, the adequate size of the carrier was confirmed by inserting a #40 verifier to the predetermined working length. Thermafil obturator #40 was selected, and the rubber stopper was set to the working length. The obturator was heated in a Thermaprep Oven (Dentsply Tulsa Dental Specialties), with the 30–60 obturator size selected, then slowly inserted into the root canal to the established working length and maintained under light apical pressure for 8 s. After cooling of the gutta-percha, the obturator was cut level with the root canal orifice using a #4 high-speed round bur, and excess gutta-percha was removed with a spoon excavator.
GuttaCore Group: Obturation was carried out as for the Thermafil group. The procedure differed in the use of a GuttaCore system #40 verifier and obturator. In addition, the obturator was heated in a GuttaCore obturator oven (Dentsply Tulsa Dental Specialties) at a size 1 heat setting.
Control Group (Continuous Wave of Condensation): A medium gutta-percha cone (DiaDent Group International, Chungcheongbuk-do, Korea) was selected and its tip calibrated to fit the working length. The first stage of the technique (down-pack) involved heating the M plugger (Analytic Technology, Redmond, Wash., USA) to 250°C and inserting it in the centre of a gutta-percha cone to 5 mm short of the working length. After cooling, the plugger was reheated and removed from the root canal. The second stage (backfill) involved injecting the root canal with gutta-percha heated to 200°C (Obtura III Max; Obtura Spartan Endodontics, Earth City, Mo., USA) and compacting every 4 mm until the root canal was filled to the level of its orifice.
Radiographs were taken of each tooth to ensure the quality of the obturation procedure. The crown portion was sealed with Cavit-G temporary restoration material (3M ESPE, Seefeld, Germany). Teeth were then kept at 37°C and 100% humidity for 15 days to allow complete cure of the obturation sealer.
Retreatment Technique
All teeth were subjected to the same retreatment protocol. First, ProTaper retreatment files D1, D2 and D3 (Dentsply Tulsa Dental Specialties) were used to remove coronal, mid-root and apical filling, respectively, until files reached the established working length. A ProMark (Dentsply Tulsa Dental Specialties) electric motor was used at a continuous rotation speed of 500 rpm for the D1 file and 400 rpm for the D2 and D3 files, using a torque setting of 3 N·cm in all cases. Files were cleaned after each use to prevent blockage of the root canal with dentin debris, and procedures were repeated as long as filling material could be seen between the cutting blades. After 5 uses, files were discarded. Canals were irrigated with 2 mL of 6% sodium hypochlorite at each instrument change using a syringe and 30-gauge needle (NaviTip, Ultradent Products) inserted to 2 mm short of the working length.
On conclusion, each tooth was examined with a dental operating microscope and radiographed. If sealer or filling debris was present, teeth were reinstrumented using hand files and a step-back approach until a #50 K-type file reached the original working length. This step was considered complete when no filling material debris was evident on the files after reinstrumentation. The samples were once again radiographed and examined under 8× magnification. If debris was still evident in the root canal, a PUENDO inserts (ProUltra EndoTip, Dentsply Tulsa Dental Specialties) were used on a ProUltra ultrasonic unit (Dentsply Tulsa Dental Specialties) set to a power level of 3. An insert was used for 30 s, followed by a 15-s pause to avoid excessive heat at the root. Irrigation was not used at this stage to allow a better view of the whole procedure. A PUENDO 3 insert was used in the cervical and middle thirds whereas a PUENDO 4 insert was used in the apical third. The cleaning process was considered complete when no further debris was detected visually. The canals were given a final flush with 5 mL of 17% EDTA, agitated for 1 minute with the EndoActivator followed by a flush with 5 mL of 6% sodium hypochlorite.
Total retreatment time for each tooth sample was recorded in seconds. It was calculated as the time spent using the rotary and hand files to reach the set working length to the point where no further debris was evident; including time spent using the ultrasonic inserts. Time taken to irrigate, change and clean instruments was excluded.
Assessment
The teeth were grooved in the buccolingual direction using a diamond disc and cleaved longitudinally with a rongeur (Fig. 1). Each sample was codified and photographed in the same position with a camera (EOS Rebel 3Ti, Canon, Melville, NY, USA) adapted for use with the dental operating microscope at 5× magnification. Assessment of the total area of the root canal and of the area containing residual filling material was carried out using imaging software (Image J 1.46r, National Institutes of Health, Bethesda, Md., USA). Values were expressed in pixels/mm and quantified by 2 independent precalibrated evaluators who were blind to the study.
 Figure 1: Example of a longitudinally cleaved tooth showing residual filling material.
Figure 1: Example of a longitudinally cleaved tooth showing residual filling material.
Statistical Analysis
The ANOVA F-test with the Tamhane multiple comparison test was used to evaluate the numeric variables studied. Levene's F-test was used to verify the hypothesis of equality of variances. The concordance correlation coefficient was used to check concordance between evaluators. The margin of error was 5% at a 95% confidence interval.
Data were keyed into an Excel spreadsheet and statistical calculations performed using SPSS version 17 (Statistical Package for the Social Sciences) and MedCalc version 11.2.0 software.
Results
The mean time required to remove filling material was significantly greater in the Thermafil group than in both the GuttaCore and control groups (p < 0.001); no significant difference was found between the latter 2 groups (Fig. 2).
Figure 2: Mean filling removal times for the Thermafil (TF), GuttaCore (GC) and control (continuous wave of condensation: CWC) groups. Means followed by the same letter are not significantly different. 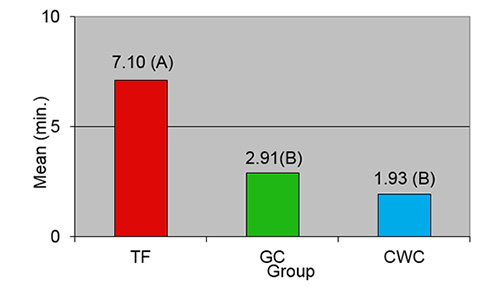
There was concordance between the 2 evaluators in quantifying the total area and residual filling material on the root canal walls. The averages of both estimates were used. No significant difference in total root canal area was observed among the groups (p > 0.05). Similarly, no significant difference in residual filling material on root canal walls was observed among the groups (p > 0.05) (Table 1).
| Parameter | TF (n = 15) |
GC (n = 15) |
CWC (n = 15) |
All groups (n = 45) |
p value* |
|---|---|---|---|---|---|
| *Using F test. | |||||
| Mean | 8.31 | 6.27 | 8.68 | 7.75 | 0.161 |
| Median | 7.81 | 5.95 | 7.79 | 7.35 | |
| Standard deviation of mean | 3.26 | 3.46 | 4.15 | 3.72 | |
| Coefficient of variation (SD/mean × 100%) | 39.23 | 55.18 | 47.81 | 48.00 | |
| Minimum | 3.91 | 1.41 | 3.08 | 1.41 | |
| Maximum | 13.41 | 13.37 | 20.40 | 20.40 | |
Discussion
Effective cleaning of the root canal system and preservation of the original anatomy of the root canal are key factors in successful endodontic retreatment.16 Residual filling material can trap remnants of necrotic tissue and microorganisms, potentially leading to treatment failure.17,18 Therefore, no resources should be spared to ensure effective removal of all filling material debris.
A number of techniques have been proposed for removing root canal filling material: the use of nickel–titanium rotary files,19 stainless steel hand files,20 ultrasound inserts21 and solvents.22,23 In the present study, a hybrid method, included the following techniques, was used for all samples: rotary files, hand files and ultrasound inserts with the aid of a dental operating microscope.
The use of ProTaper retreatment files is an efficient method for removing filling material,24 but this technique alone may not suffice.25 A final stage to complete the process and carry out further instrumentation of the root canal is necessary.13,25 We used hand files for this finishing procedure, which yielded filling material debris, thereby confirming the importance of this supplementary work.
No solvent was used to aid filling removal. In 2009, Takahashi and colleagues26 noted that the use of ProTaper retreatment files for gutta-percha removal was quicker without the use of a solvent. In addition, chemical melting of gutta-percha leaves a thin layer that can adhere to canal walls27 or be forced into the isthmus, lateral canals and irregularities,28 complicating the root canal cleaning process.
The method adopted here provided clinical confirmation of the utility of an operating microscope to visualize residual filling material after instrumentation. Subsequent removal of residual material by ultrasound vibration suggested cleanliness. This observation corroborates the findings of the study by Mello Jr. and colleagues,29 who showed improved efficacy in removing filling material from root canal walls with the supplementary use of ultrasound inserts and an operating microscope. However, the use of an operating microscope is limited when canals are curved. Moreover, it is important to reiterate that ultrasonic inserts should be used with caution, particularly in the apical portion of the canal, to safeguard against damage such as perforation or weakening of the tooth structure when excessive dentin removal is performed using ultrasonic inserts.10
Shortening clinical times and enhancing procedural efficacy remain a constant challenge in the field of endodontics. In the present study, retreatment time for the samples filled with Thermafil was significantly longer than for those filled with GuttaCore or continuous wave of condensation (control group). In 2013, Beasley and others13 also observed longer retreatment time with Thermafil compared with GuttaCore. However, despite the significant difference, this may not be relevant clinically. The increased time required was attributed to greater difficulty in removing the plastic carrier. According to Wilcox,30 "Adequacy of Thermafil retreatment may be related more to the ability to easily remove the carrier than to the technique of gutta-percha removal."
We used maxillary central incisors as they have a straight root canal and allow reproducible clinical conditions in a laboratory study. According to Zuolo and colleagues,31 these teeth are widely used in research using the methods applied in this study.
For sample assessment, roots were cleaved longitudinally and submitted to quantitative analysis, according to widely used methods.19,26,29,31 Before cleaving, all teeth were radiographed and examined using a dental operating microscope to simulate clinical conditions of assessment of the absence of filling material. However, cleaving of the roots exposed traces of debris on root canal walls of all samples. Previous studies have revealed the same finding, irrespective of material or method used for filling removal,12,21,26,29 and a prior study13 evaluated the time required to remove GuttaCore, Thermafil Plus and thermoplasticized gutta-percha from the root canals. This is the first study comparing residual filling material after root canal retreatment among the GuttaCore and Thermafil carriers. Results revealed no significant difference among the groups regarding efficiency of filling material removal and suggested no difference in efficiency in removing gutta-percha with or without carrier.
The results of this study indicate that GuttaCore can be removed faster than Thermafil filling. Moreover, the finding of residual filling material on root canal walls of all samples illustrates that effective retreatment remains an ongoing challenge in the endodontic field.
THE AUTHORS
 |
Dr. Nevares is PhD student in department of operative dentistry and endodontics, Dental College of Pernambuco, University of Pernambuco, Camaragibe, PE, Brazil. |
 |
Dr. de Albuquerque is associate professor in department of operative dentistry and endodontics, Dental College of Pernambuco, University of Pernambuco, Camaragibe, PE, Brazil. |
 |
Dr. Zuolo is part time professor in endodontics,, School of Professional Development, State of São Paulo Dental Association (EAP-APCD), São Paulo, SP, Brazil. |
 |
Dr. Bueno is professor and department head, Dental Research Center, São Leopoldo Mandic Faculty, Campinas, SP, Brazil. |
 |
Dr. Cunha is associate professor and department head, Restorative Dentistry College of Dentistry, Faculty of Health Sciences, University of Manitoba, Winnipeg, Manitoba. |
The authors have no declared financial interests.
This article has been peer reviewed.
Correspondence to: Dr. Giselle Nevares, Department of Operative Dentistry and Endodontics, Dental College of Pernambuco, University of Pernambuco, Avenida Gal Newton Cavalcanti, 1650, Tabatinga, ZIP: 54753-901, Camaragibe, PE, Brazil. Email: gnevares@yahoo.com
References
- Rhome BH, Solomon EA, Rabinowitz JL. Isotopic evaluation of the sealing properties of lateral condensation, vertical condensation, and Hydron. J Endod. 1981;7(10):458-61.
- Tagger M, Tamse A, Katz A, Korzen BH. Evaluation of the apical seal produced by a hybrid root canal filling method, combining lateral condensation and thermatic compaction. J Endod. 1984;10(7):299-303.
- Buchanan LS. The continuous wave of obturation technique: 'centered' condensation of warm gutta percha in 12 seconds. Dent Today. 1996;15(1):60-2, 64-7.
- De-Deus G, Reis C, Beznos D, de Abranches AM, Coutinho-Filho T, Paciornik S. Limited ability of three commonly used thermoplasticized gutta-percha techniques in filling oval-shaped canals. J Endod. 2008;34(11):1401-5.
- Marciano MA, Ordinola-Zapata R, Cunha TV, Duarte MA, Cavenago BC, Garcia RB, et al. Analysis of four gutta-percha techniques used to fill mesial root canals of mandibular molars. Int Endod J. 2011;44(4):321-9.
- Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965;20:340-9.
- Delivanis PD, Mattison GD, Mendel RW. The survivability of F43 strain of Streptococcus sanguis in root canals filled with gutta-percha and Procosol cement. J Endod. 1983;9(10):407-10.
- Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J. 2001;34(1):1-10.
- Nair PN. On the causes of persistent apical periodontitis: a review. Int Endod J. 2006;39(4):249-81.
- Ruddle CJ. Nonsurgical retreatment. J Endod. 2004;30(12):827-45.
- Johnson WB. A new gutta-percha technique. J Endod. 1978;4(6):184-8.
- Zuolo ML, Imura N, Ferreira MO. Endodontic retreatment of Thermafil or lateral condensation obturations in post space prepared teeth. J Endod. 1994;20(1):9-12.
- Beasley RT, Williamson AE, Justman BC, Qian F. Time required to remove GuttaCore, Thermafil Plus, and thermoplasticized gutta-percha from moderately curved root canals with ProTaper files. J Endod. 2013;39(1):125-8.
- Grossman LI. Endodontic Practice. 8th ed. Philadelphia: Lea & Febiger; 1974. p. 299-300.
- Declaration of Helsinki. Ferney-Voltaire, France: World Medical Association. Available: http://www.wma.net/en/30publications/10policies/b3/ (accessed 2015 Oct. 12).
- Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod. 2004;30(1):1-4.
- Stabholz A, Friedman S. Endodontic retreatment — case selection and technique. Part 2: Treatment planning for retreatment. J Endod. 1988;14(12):607-14.
- Saad AY, Al-Hadlaq SM, Al-Katheeri NH. Efficacy of two rotary NiTi instruments in the removal of gutta-percha during root canal retreatment. J Endod. 2007;33(1):38-41.
- Marques da Silva B, Baratto-Filho F, Leonardi DP, Henrique Borges A, Volpato L, Branco Barletta F. Effectiveness of ProTaper, D-RaCe, and Mtwo retreatment files with and without supplementary instruments in the removal of root canal filling material. Int Endod J. 2012;45(10):927-32.
- Imura N, Zuolo ML, Ferreira MO, Novo NF. Effectiveness of the Canal Finder and hand instrumentation in removal of gutta-percha root fillings during root canal retreatment. Int Endod J. 1996;29(6):382-6.
- Pirani C, Pelliccioni GA, Marchionni S, Montebugnoli L, Piana G, Prati C. Effectiveness of three different retreatment techniques in canals filled with compacted gutta-percha or Thermafil: a scanning electron microscope study. J Endod. 2009;35(10):1433-40.
- Wilcox LR. Endodontic retreatment with halothane versus chloroform solvent. J Endod. 1995;21(6):305-7.
- Cunha RS, De Martin AS, Barros PP, da Silva FM, Jacinto RC, Bueno CE. In vitro evaluation of the cleansing working time and analysis of the amount of gutta-percha or Resilon remnants in the root canal walls after instrumentation for endodontic retreatment. J Endod. 2007;33(12):1426-8.
- Gu LS, Ling JQ, Wei X, Huang XY. Efficacy of ProTaper Universal rotary retreatment system for gutta-percha removal from root canals. Int Endod J. 2008;41(4):288-95.
- Huang X, Ling J, Wei X, Gu L. Quantitative evaluation of debris extruded apically by using ProTaper Universal Tulsa rotary system in endodontic retreatment. J Endod. 2007;33(9):1102-5.
- Takahashi CM, Cunha RS, de Martin AS, Fontana CE, Silveira CF, da Silveira Bueno CE. In vitro evaluation of the effectiveness of ProTaper Universal rotary retreatment system for gutta-percha removal with or without a solvent. J Endod. 2009;35(11):1580-3.
- Sae-Lim V, Rajamanickam I, Lim BK, Lee HL. Effectiveness of ProFile .04 taper rotary instruments in endodontic retreatment. J Endod. 2000;26(2):100-4.
- Kfir A, Tsesis I, Yakirevich E, Matalon S, Abramovitz I. The efficacy of five techniques for removing root filling material: microscopic versus radiographic evaluation. Int Endod J. 2012;45(1):35-41.
- de Mello Jr JE, Cunha RS, Bueno CE, Zuolo ML. Retreatment efficacy of gutta-percha removal using a clinical microscope and ultrasonic instruments: part I — an ex vivo study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(1):e59-62.
- Wilcox LR. Thermafil retreatment with and without chloroform solvent. J Endod. 1993;19(11):563-6.
- Zuolo AS, Mello Jr JE, Cunha RS, Zuolo ML, Bueno CE. Efficacy of reciprocating and rotary techniques for removing filling material during root canal retreatment. Int Endod J. 2013;46(10):947-53.