
ABSTRACT
Open-field aluminum–nickle–cobalt magnets have been used in prosthodontics for many years, but success has been limited because these magnets are susceptible to corrosion by the saliva and because their retentive force is weak relative to the initial retention offered by mechanical attachments. More recently, magnets have been made from alloys of the rare earth elements samarium and neodymium, which provide stronger magnetic force per unit size. In addition, a new generation of laser-welded containers has improved protection from salivary corrosion. The current resurgence of interest in this type of attachment appears justified because, unlike mechanical attachments, magnets have potential for unlimited durability and might therefore be superior to mechanical ball or bar attachments for the retention of removable prostheses on implants. To date, no long-term prospective trials have been conducted to confirm the clinical durability of this new generation of magnets for retaining dentures on either teeth or implants. The aim of this study was to document initial clinical experiences and levels of satisfaction among edentulous patients treated with mandibular implant-supported overdentures retained using a new generation of rare-earth magnetic attachments. At the outset, all but one of the 17 patients had had several years of experience with implant-supported overdentures. During the first year, the mean overall satisfaction among these 17 patients increased from less than 70 to over 90 out of 100 (standardized visual analogue scale). No unusual difficulties were encountered in rendering the treatment or maintaining the attachments. This report offers preliminary evidence of the excellent potential of these magnets for retaining mandibular implant-supported overdentures.
Introduction
Magnets made from aluminum–nickle–cobalt (AlNiCo) alloys have been used in dentistry for many years.1 Initially, the repellent force of like magnetic poles was harnessed from open-field AlNiCo alloys embedded in the base of upper and lower dentures, so that the repellent forces would keep dentures on the residual ridges. However, this approach achieved little popularity because the force was weak, and the direction of the force was just as likely to repel the dentures out of the mouth. A more popular method was to attach a ferromagnetic metal keeper (generally made of stainless steel) to the tooth or implant for attraction by a magnet embedded in the nearby denture base; this arrangement is known as a magnet–keeper unit. Others used surgery to place a magnetic implant within the jaw, which would then attract the magnet in the denture base.2 However, these clinical approaches lost popularity, particularly when clinicians discovered that AlNiCo alloys corrode rapidly in saliva. In summary, these older open-field magnet systems corroded easily3 and their attractive force was weaker (mean of 2 N or less) than that of mechanical attachments used to retain dentures, such as ball or bar attachments.4 This paper briefly reviews recent improvements in the magnet alloys used in prosthodontics and reports patients’ satisfaction with magnet-retained mandibular implant overdentures 1 year after placement.
Recent Developments
Newer magnetic systems have been made available for prosthodontics in the past couple of decades with the introduction of alloys of the rare earth elements samarium (SmCo) and, more recently, neodymium (NdFeB) in closed-field systems. Rare-earth alloys produce a stronger and more stable magnetic force than was previously available because they have high magnetization and high resistance to demagnetization.1 In closed-field systems, the magnetic field or flux is contained within the magnet–keeper unit and yields a much greater attractive force per unit size than is possible with open-field systems. The magnetic force permeates the closed-field system with much less resistance than occurs in the surrounding air. Therefore, the strength of magnetism or the “density of flux” is concentrated between the north and south poles of the magnet. The newer closed-field magnets also have a higher attractive force per unit size when the keeper and the magnet are in contact, although this force diminishes rapidly when the magnet and keeper lose contact.5,6 Overall, the magnetic circuit in a closed-field dental attachment is nearly 4 times stronger (mean of 5.8 N or greater; dome type = 600 gf [gram force] or 5.88 N) than older open-field circuits, and leakage of magnetic flux from the closed circuit is less. In general, the lifespan of a magnetic force is infinite, which means that the retentive force of a magnetic unit should be maintained long after distortion has occurred in mechanical attachments.4 Moreover, the magnetic unit offers little lateral resistance to displacement, which reduces the potentially damaging lateral force directed by a denture onto a tooth or implant.7
In addition, a new system has been introduced to seal the metal capsule around a magnet and thus to protect it from corrosion in the mouth. According to one manufacturer (MAGFIT, Aichi Steel Corporation, Aichi, Japan) the integrity of the system is assured by carefully micro laser welding the 2 parts of the capsule together to a depth of about 70 µm.8,9 The parts are made of 19Cr–2 Mo–0.1Ti magnetic stainless steel and they are laser welded together with a narrow bead of 16Cr–12Ni–2Mo non-magnetic stainless steel containing 12% nickel. According to the manufacturer, fewer than 1 in 10 capsules associated with overdentures on natural teeth separated from the denture base during an 8-year clinical trial; more interestingly, none experienced loss of magnetic attraction.9 The manufacturer also reported that a 3-µm veneer of ceramic titanium nitride was applied to the container to resist abrasion and reduce the patient’s exposure to nickel.10 Nonetheless, until there is stronger evidence to support these claims, it would be prudent to avoid this magnetic system for patients with an allergy to nickel.
Patient Satisfaction
In a 10-year randomized clinical trial, there was no difference in general satisfaction with an older open-field magnetic attachment system for retaining mandibular complete dentures and 2 types of mechanical attachments (ball or bar systems).11 After 10 years, regardless of the attachment system used, the patients rated overall satisfaction with their lower prostheses at about 8 on a scale of 1 to 9, where 9 was “excellent.” However, in that trial and the 2 other randomized trials involving magnets (short-term crossover studies that also used older open-field magnet systems),12,13 the dentures retained by magnets were subjectively less stable and less comfortable than dentures retained by mechanical attachments. Despite these subjective impressions, there was no difference in satisfaction among patients with different attachment types. The magnetic dentures in the 10-year trial11 had a mean retentive force of 3–4 N for 2 implants combined (mean of less than 2 N per implant), which was significantly lower than the initial retentive force of the mechanical attachments. Furthermore, in this same trial, the magnet-retained dentures required substantially more maintenance, including replacement of the magnets approximately twice as often (or more) as was required for the mechanical attachments. The usual reason for replacing the magnets was wear and corrosion. The incongruity between maintenance problems with the magnets and high patient satisfaction may simply reflect the fact that the patients likely received a high level of care in the context of the study. The apparent lack of difference in satisfaction between groups after 10 years might also have been related to the format of the comparisons, which were based on patients’ original group assignments, even though patients with magnets were more likely than patients in the other groups to change to a different attachment system during the study. At any rate, satisfaction with a stronger and more durable magnet system might be more sustainable than satisfaction with mechanical attachments over time if the retention of the magnetic system surpasses that provided by mechanical attachments.
Hygiene and Periodontal Findings
Clinical evidence over 10 years,14 corresponding to the current authors’ observations over 1 year in the study reported below, indicates that mechanical and magnetic attachments do not disturb the surrounding gingiva or periodontium. In shorter-term trials, there have been reports of more microbial plaque collecting around magnetic attachments than around mechanical attachments,15,16 but there has been no reasonable explanation for this observation. Assad and colleagues15 suggested that magnets attract microbial plaque, but it has also been suggested that because of its emergence profile, the magnetic keeper may trap plaque around the implant where it emerges from the mucosa16 or that denture-wearers who were dissatisfied with the retention of their dentures were not motivated to keep them clean.14
Other Attributes
Magnetic attachments used to retain dentures are typically shorter than mechanical attachments, which is particularly useful for patients with restricted interocclusal space and challenging esthetic demands. Magnetic attachments can also accommodate a moderate divergence of alignment between 2 or more abutments, since they do not depend on a particular path of insertion; in this respect, magnetic attachments are unlike most mechanical attachments, which generally require minimal divergence for best function. Furthermore, patients with physical disabilities such as those experienced by frail older adults, have reported that magnet-retained dentures are relatively easy to place and remove.17,18
Magnetic Resonance Imaging
Magnets and even the ferromagnetic stainless steel keeper may cause distortion during magnetic resonance imaging (MRI) of the head and neck.19 It is therefore recommended that patients remove dentures with magnets and have the keepers unscrewed from the implants before an MRI investigation of the region. As with most metallic dental materials, there is minimal risk of patient injury through displacement of the keeper component during MRI, provided the keepers are properly attached within the mouth.20
Initial Clinical Report of Magnet-Retained Dentures
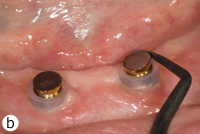
 Figure 1: Clinical appearance 1 year after attachment of denture with magnets.
Figure 1: Clinical appearance 1 year after attachment of denture with magnets.


Figure 2: a) Magnet (on top) with keeper (abutment and screw) and b) assembled magnet-keeper unit.
We present here a preliminary 1-year clinical report from a case series of implant-retained dentures, in which the benefits and limitations of a rare-earth magnetic system (MAGFIT) were monitored. The primary objective of the study was to determine the satisfaction of patients who used complete dentures retained by rare-earth magnets supported on 2 implants in the mandible. Approval to test the magnet system was obtained from Health Canada, and approval for the clinical study was obtained from the Clinical Research Ethics Board of the University of British Columbia.
Materials and Methods
Consecutive patients with complete implant-supported overdentures in the mandible who were attending a university dental clinic were recruited for the study starting in December 2006. All had been edentulous for many years. All but one of the patients had previous experience with mechanical ball or bar attachments to retain their lower dentures on 2 implants over at least 3 years before being considered for the study. The remaining patient had had 2 implants placed 4 months before recruitment, but they had not yet been attached to her lower denture. Potential study participants were excluded if their general health was unstable or if the complete dentures they wore were clinically unacceptable according to any standard clinical criteria other than retention.21 The implants for all patients were threaded titanium screws made by Nobel Biocare (Nobel Biocare Canada Inc., Richmond Hill, ON) or Straumann (Straumann Canada Ltd., Burlington, ON). Treatment in the study was provided at no financial cost to the patients.
Each patient included in the study had 2 separate magnetic attachments associated with 2 implants serving to retain a mandibular complete denture. Magnet keepers were screwed into place on the implants and were tightened to about 30 N/cm. The height of the keepers was selected to remain above the mucosa (Fig. 1). The opposing surfaces of the keeper component and the magnetic capsule are domed to allow them to rotate and pivot on one another as the denture moves on the mucosa of the residual ridge (Figs. 2a and 2b). The magnetic capsules were placed on the keepers and attached to the denture base intraorally with autopolymerizing methylmethacrylate (Orthodontic Resin, Dentsply Caulk, Milford, DE) (Figs. 3a–3e). Each patient was asked to rate overall satisfaction using a standardized visual analogue scale (VAS) at baseline, 6 months and 1 year, with level of satisfaction being indicated as a crossed mark on a scale from 1 mm (very unsatisfied) to 100 mm (very satisfied).22
 |
 |
 |
 |
 |
Figure 3: Clinical application of MAGFIT magnetic attachment: a) the keeper abutments are placed on the implants; b) the magnet capsules are positioned on the keepers; c) acrylic resin is added to attach the magnets; d) resin extruded during intraoral placement of the denture; e) magnets are attached to the denture base.
Results
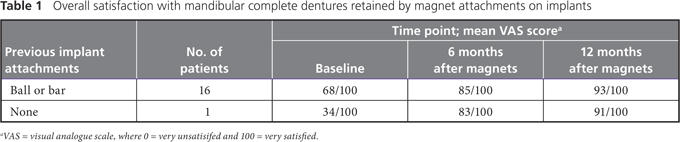
At the time of writing, in late 2009, the first 17 consecutively treated patients had at least 1 year of experience with magnet-retained overdentures. Among the 16 patients who presented with existing mechanical ball or bar attachments, the mean overall VAS satisfaction score was 68 out of 100 at baseline (before placement of the magnetic attachments) and rose to 93 after 12 months (Table 1). The patient with no previous experience with implant attachments reported a baseline VAS score of 34 for the lower denture; the score rose dramatically (to 91) by the end of the first year.
Discussion
From this small clinical study, we can infer that the patients were very satisfied in the short-term with use of a magnet system to retain complete dentures on implants in the mandible. Notably, most of the patients had experienced mechanical attachments for several years before placement of the magnet system and had been relatively satisfied with the result. The baseline VAS score for the 16 patients who had experience with implant-supported dentures (68 out of 100), was lower than the mean satisfaction scores after 3 years in a recent comparison of different mechanical attachments (ball or bar designs) for mandibular implant-supported overdentures.22 In that study, mean satisfaction scores exceeded 90 out of 100, despite a relatively high incidence of abrasion or breakage of the mechanical components in the group with ball attachments. Rare-earth alloys provide considerably more magnetic force per unit size than their predecessors, and new laser-welding techniques contribute to the construction of strong and durable containers for protecting the magnets from salivary corrosion. However, no clinical data are yet available for this newer magnet system, other than what the manufacturer has provided. Because the durability of magnetic attachments remains unknown beyond 1 year, we will continue to monitor these patients and others for several years.
These 1-year results show excellent patient satisfaction with magnet-retained mandibular overdentures – certainly no less than the satisfaction of the same patients with mechanical attachments over several years (as indicated by baseline VAS scores). Furthermore, there were no unusual technical difficulties in rendering the treatment or maintaining the implants. As in our previous study with mechanical attachments,22 there was one patient in whom the magnet separated from the denture base during the first year, for which reattachment using autopolymerizing methylmethacrylate was required. By the end of the first year, no corrosion of magnets was observed clinically. Also, no patients required repair or relining of their implant dentures during the year, and all reported ease in maintaining their mouth and denture hygiene. Of course, potential problems with the magnets may exist, ranging from uncertainty about long-term protection from salivary corrosion within the protective capsules to the potential for distortion of images if patients undergo MRI of the head and neck. Given the clinical experience reported here, the current resurgence of interest in magnet-retained implant-supported overdentures appears justified, especially when mechanical attachments have failed to fully satisfy a patient’s expectations.
Conclusion
Magnetic attachments can be used to retain mandibular implant overdentures. In a small case series, patient satisfaction over the first year was excellent, especially for patients who had been less than satisfied with mechanical attachments. This new generation of magnetic attachment can be applied in a straightforward manner and offers the potential for long-term durability.
THE AUTHORS
|
Dr. Ceruti is an assistant professor of oral and maxillofacial rehabilitation and oral implants, University of Torino, Torino, Italy. |
|
|
Dr. Bryant is an assistant professor of prosthodontics and dental geriatrics, faculty of dentistry, University of British Columbia, Vancouver, British Columbia. Email: rbryant@interchange.ubc.ca |
|
|
Dr. Lee is a private dental practitioner in Seoul, Korea. |
|
|
Dr. MacEntee is a professor of prosthodontics and dental geriatrics, faculty of dentistry, University of British Columbia, Vancouver, British Columbia. |
Acknowledgements: The clinical experience described in this paper was gained by the authors through a grant from Aichi Steel Corporation, Japan. The authors alone are solely responsible for the content of the paper and their opinions and conclusions are not influenced in any way by Aichi Steel Corporation. Ethical approval granted by the University of British Columbia Clinical Research Ethics Board (C06-0042).
Correspondence to: Dr. Ross Bryant, Faculty of dentistry, University of British Columbia, 2199 Wesbrook Mall, Vancouver, BC V6T 1Z3.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- Riley MA, Walmsley AD, Harris IR. Magnets in prosthetic dentistry. J Prosthet Dent. 2001;86(2):137-42.
- Behrman SJ, Egan G. Implantation of magnets in the jaw to aid denture retention. N Y State Dent J. 1953;19:353-71.
- Riley MA, Williams AJ, Speight JD, Walmsley AD, Harris IR. Investigations into the failure of dental magnets. Int J Prosthodont. 1999;12(3):249-54.
- Saygili G, Sahmali S. Retentive forces of two magnetic systems compared with two precision attachments. J Oral Sci. 1998;40(2):61-4.
- Akaltan F, Can G. Retentive characteristics of different dental magnetic systems. J Prosthet Dent. 1995;74(4):422-7.
- Highton R, Caputo AA, Pezzoli M, Matyas J. Retentive characteristics of different magnetic systems for dental applications. J Prosthet Dent. 1986;56(1):104-6.
- Tokuhisa M, Matsushita Y, Koyano K. In vitro study of a mandibular implant overdenture retained with ball, magnet, or bar attachments: comparison of load transfer and denture stability. Int J Prosthodont. 2003;16(2):128-34.
- Ishikawa M, Kashiwabara T, Ishida O, Ichikawa T. Installing magnetic keepers using LASER welding. J Prosthodont. 2002;11(1):49-52.
- Hiroshi I. Clinical analysis on the reliability of the magnetic attachment over an 8 year period. In: Ai M, Shiau YY, editors. New magnetic applications in clinical dentistry. Tokyo: Quintessence International; 2004. p. 93-6.
- Honkura Y. The new generation of dental magnetic attachment. In: Ai M, Shiau YY, editors. New magnetic applications in clinical dentistry. Tokyo: Quintessence International; 2004. p. 51-56.
- Naert I, Alsaadi G, Quirynen M. Prosthetic aspects and patient satisfaction with two-implant-retained mandibular overdentures: a 10-year randomized clinical study. Int J Prosthodont. 2004;17(4):401-10.
- Cune M, van Kampen F, van der Bilt A, Bosman F. Patient satisfaction and preference with magnet, bar-clip, and ball-socket retained mandibular implant overdentures: a cross-over clinical trial. Int J Prosthodont. 2005;18(2):99-105.
- Burns DR, Unger JW, Elswick RK Jr, Giglio JA. Prospective clinical evaluation of mandibular implant overdentures: Part II – Patient satisfaction and preference. J Prosthet Dent. 1995;73(4):364-9.
- Naert I, Alsaadi G, van Steenberghe D, Quirynen M. A 10-year randomized clinical trial on the influence of splinted and unsplinted oral implants retaining mandibular overdentures: peri-implant outcome. Int J Oral Maxillofac Implants. 2004;19(5):695-702.
- Assad AS, Abd El-Dayem MA, Badawy MM. Comparison between mainly mucosa-supported and combined mucosa-implant supported mandibular overdentures. Implant Dent. 2004;13(4):386-94.
- Davis DM, Packer ME. Mandibular overdentures stabilized by Astra Tech implants with either ball attachments or magnets: 5-year results. Int J Prosthodont. 1999;12(3):222-9.
- Allen PF, Ulhuq A, Kearney J. Strategic use of a new dental magnet system to retain partial and complete overdentures. Eur J Prosthodont Restor Dent. 2005;13(2):81-6.
- Chu FC, Deng FL, Siu AS, Chow TW. Implant-tissue supported, magnet-retained mandibular overdenture for an edentulous patient with Parkinson's disease: a clinical report. J Prosthet Dent. 2004;91(3):219-22.
- Laurell KA, Gegauff AG, Rosenstiel SF. Magnetic resonance image degradation from prosthetic magnet keepers. J Prosthet Dent. 1989;62(3):344-8.
- Gegauff AG, Laurell KA, Thavendrarajah A, Rosenstiel SF. A potential MRI hazard: forces on dental magnet keepers. J Oral Rehabil. 1990;17(5):403-10.
- MacEntee MI. The complete denture: a clinical pathway. Carol Stream (ILL): Quintessence International; 1999.
- MacEntee MI, Walton JN, Glick N. A clinical trial of patient satisfaction and prosthodontic needs with ball and bar attachments for implant-supported complete overdentures: three-year results. J Prosthet Dent. 2005;93(1):28-37.