ABSTRACT
Developmental disturbances of permanent teeth can result from trauma to primary teeth because of the proximity of the root of the primary teeth to their permanent successors. We describe the case of a 14-month-old boy who was referred to the baby clinic of the School of Dentistry, Universidad Estadual Paulista, Araçatuba, Brazil, after sustaining a severe trauma that led to intrusion of the right primary central incisor. Radiographic examination 4 years after the trauma showed a developing morphological change in the germ of the permanent successor. On eruption of the permanent central incisor, a crown malformation along with enamel hypoplasia was observed. We conclude that radiographic follow-up is indicated after trauma to monitor possible sequelae in the permanent successors even before their eruption.
Introduction
Traumatic injuries to primary teeth occur with high frequency—in 15% to 30% of children.1,2 Small coronal fractures may be observed, although luxations are more common because of the pliability of the facial skeleton and periodontal ligament, the large volume of teeth in relation to the bone in primary and mixed dentition, and the shorter roots of primary teeth.3
Disturbances in the developing germs of permanent incisors after a trauma to the primary dentition are usually related to intrusive injuries.4,5 An intrusive injury is the consequence of impact in an axial direction that results in displacement of the tooth within the socket.6 The prevalence of developmental disturbances to permanent teeth secondary to intrusive injury to primary dentition is 18%–69%.4,7
Severe intrusion by primary tooth and invasion of the developing germ during the earliest phases of odontogenesis, when the child is aged 1–3 years, may result in malformation of the permanent tooth germ.4,8 This is when the formation of the medial and incisal thirds of the enamel matrix of the permanent tooth takes place. Moreover, displacement of the primary tooth root may affect development of the permanent tooth by altering the secretory phase of the ameloblasts5 or, in subsequent stages, by affecting the root formation process.7
In diagnosing and treating traumatic injuries to primary teeth, the aim is to deal with pain and to prevent sequelae in the developing permanent tooth germ.4,7 There is no agreement on the ideal treatment of deciduous intruded teeth after trauma. To date, treatment has been based on clinical case reports,9,10 expert opinion11,12 and literature review.7,13-16
The purpose of this article is to present a case of oral trauma in the primary dentition and its consequences for the formation of developing permanent germs.
Case Report
A 14-month-old boy was referred to the baby clinic of the School of Dentistry, Universidad Estadual Paulista, Araçatuba, Brazil, 20 minutes after he suffered a dental trauma. The child was in good general health and had no neurologic problems. The child's parents reported that he had fallen on the floor.
Intraoral examination revealed a blood clot in the alveolar region of the upper right deciduous central incisor (tooth 51) and extensive laceration of the palatine mucosa (Fig. 1a). On palpation, a hardened surface was observed in the lingual area. Radiographic examination (Fig. 1b) showed that tooth 51 had suffered severe intrusion and lingual luxation.
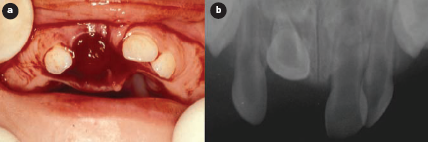
Figure 1: Initial examination: a) clinical view of the traumatized area; b) radiographic aspect of the intruded tooth.
The patient received local infiltrative anesthesia on the labial and buccal side of the tooth and the tooth was repositioned in a labial direction by digital pressure. The clot was then removed, revealing the crown of the intruded tooth. Tissue closure was performed by proximal suture of the affected tooth. It was decided to retain the traumatized tooth. Clinical and radiographic examinations were carried out periodically to monitor tooth development.
A week later, the mucosa had almost healed and the tooth displayed mild mobility. Radiographic examination showed no alterations. After 12 months, clinical examination revealed no discoloration of the dental crown or pain, and the mucosa presented normal characteristics (Fig. 2a). Radiographic examination did not show any alterations (Fig. 2b).

Figure 2: Clinical and radiographic views, 1 year after trauma: a) clinical examination revealed normal mucosa and no discoloration of the dental crown; b) radiographic examination showed normal characteristics.
After 4 years, signs of alteration of the germ of the maxillary right central permanent incisor were observed radiographically (Fig. 3), and the parents were informed of morphological alterations in the permanent tooth. Clinical examination 6 years after the trauma revealed that the permanent maxillary right central incisor (tooth 11) had erupted into the oral cavity. There was evidence of malformation, discoloration and dilaceration of the crown (Figs 4a and 4b). The defect was restored with a light-cured composite resin.

Figure 3: Radiographic examination 4 years after dental trauma revealed signs of alteration in the germ of the maxillary right central permanent incisor.
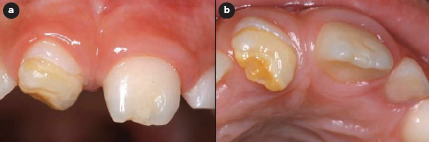
Figure 4: Crown malformation of the permanent teeth: a) intraoral view showing enamel hypoplasia on the permanent maxillary right central incisor and circular enamel hypoplasia on the permanent left central incisor; b) intraoral view showing dilaceration of the crown of tooth 11 and discoloration.
Discussion
Treatment of intrusive injuries in primary dentition includes determination of the relationship between the primary and the permanent teeth.2-4,17,18 Depending on the direction of displacement suffered by the dental element, treatment may involve waiting for spontaneous re-eruption or surgical removal of the element. Thus, if the apex is displaced toward or through the labial bone plate, the tooth is left to re-erupt spontaneously.19,20 If the apex is displaced toward the permanent tooth germ, it should be extracted.8,20 The main concern is to minimize disturbances to the development of the permanent successors.8
In the present case, several factors influenced the decision to reposition and retain the traumatized tooth: the short time elapsed before seeking treatment (20 minutes), the anxiety of the family to maintain the erupting tooth and the patient's age.
Intrusive luxation of a primary incisor often results in it being driven deeply into the alveolar bone, invading the follicle of the permanent germ, which lies palatally or lingually in close proximity to the primary incisor root21 and possibly destroying the enamel matrix, depending on the severity of the intrusion.22,23 As ameloblasts are irreplaceable and no further cell division occurs after completion of enamel formation, localized arrest of crown development is likely to occur after trauma.24
Moreover, the degree of damage to the permanent successor depends on the stage of crown formation. White discoloration is the result of accelerated deposition of minerals caused by trauma during the maturation stage of enamel development. Yellow-brown discolorations are caused by incorporation of the breakdown products of hemoglobin from bleeding in the periapical area. The destruction of ameloblasts in the active enamel epithelium results in enamel hypoplasia.7,25 In the present case, there was partial arrest of crown formation resulting in a malformed crown, enamel hypoplasia and dilaceration of the crown of tooth 11.
The age at which the trauma took place explains the sequelae noted in the permanent dentition. Formation of the tooth germ of the permanent upper central incisors takes place at 20 weeks gestation, and calcification begins at the age of 3–4 months.26 Therefore, orofacial trauma at 14 months, as in this case, could lead to discoloration and malformation. Severe dental malformation resulting from injury at this age has been described in the literature.27,28
Careful follow-up of a traumatic injury is important, to ensure that no problems arise that may cause damage to the developing permanent teeth. This case showed the importance of regular follow-up appointments. In particular, pre-eruptive radiography is recommended to allow early detection and treatment of possible severe developmental disturbances.
With regard to the malformation of the permanent tooth germ reported in this article, prior studies4,5,7,20,26,28 support our finding that intrusion injuries are the most common cause of developmental disturbances. However, crown malformations accompanied by enamel hypoplasia have not previously been classified as developmental disturbances. Turgut and colleagues29 recently reported an unusual case of developmental disturbance of an unerupted permanent incisor due to trauma to its predecessor, similar to the present case. The authors reported the presence of enamel hypoplasia with coronal malformation. Therefore, the type of traumatic primary tooth injury combined with the age of the child at the time of trauma may indicate the probability of subsequent secondary damages. Thus, the importance of accurate exploration and documentation of the trauma is apparent. Especially in cases of intrusion injuries in children 1–3 years of age, we recommend regular follow-up. Pre-eruptive radiology is particularly recommended to allow early detection and treatment of possible severe developmental disturbances.
THE AUTHORS
|
Dr. Gomes is a postgraduate student in pediatric dentistry, School of Dentistry, Universidad Estadual Paulista, Araçatuba, SP, Brazil. |
|
|
Dr. Messias is a postgraduate student in pediatric dentistry, School of Dentistry, Universidad Estadual Paulista, Araçatuba, SP, Brazil. |
|
|
Dr. Delbem is associate professor of pediatric dentistry, School of Dentistry, Universidad Estadual Paulista, Araçatuba, SP, Brazil. |
|
|
Dr. Cunha is associate professor of pediatric dentistry, School of Dentistry, Universidad Estadual Paulista, Araçatuba, SP, Brazil. |
Correspondence to: Dr. Alessandra Cristina Gomes, Department of pediatric dentistry, School of Dentistry, UNESP - São Paulo State University, Rua José Bonifácio 1193, Araçatuba, Cep 16015-050, SP – Brazil.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- Forsberg CM, Tedestam G. Traumatic injuries to teeth in Swedish children living in an urban area. Swed Dent J. 1990;14(3):115-22.
- Cunha R F, Pugliesi DM, de Mello Vieira AE. Oral trauma in Brazilian patients aged 0–3 years. Dent Traumatol. 2001;17(5):210-2.
- Cardoso M, de Carvalho Rocha MJ. Traumatized primary teeth in children assisted at the Federal University of Santa Catarina, Brazil. Dent Traumatol. 2002;18(3):129-33.
- Holan G, Ram D, Fuks AB. The diagnostic value of lateral extraoral radiography for intruded maxillary primary incisors. Pediatr Dent. 2002;24(1):38-42.
- Flores MT. Traumatic injuries in the primary dentition. Dent Traumatol. 2002;18(6):287-98.
- Arenas M, Barbería E, Lucavechi T, Maroto M. Severe trauma in the primary dentition — diagnosis and treatment of sequelae in permanent dentition. Dent Traumatol. 2006;22(4):226-30.
- Diab M, elBadrawy HE. Intrusion injuries of primary incisors. Part III: Effects on the permanent successors. Quintessence Int. 2000;31(6):377-84.
- Andreasen JO. Injuries to the developing teeth. In: Andreasen JO, Andreasen FM, editors. Textbook and color atlas of traumatic injuries to the teeth. Copenhagen: Munksgaard; 1994. p. 457-94.
- Weiger R, Heuchert T. Management of an avulsed primary incisor. Endod Dent Traumatol. 1999;15(3):138-43.
- Kinoshita S, Mitomi T, Taguchi Y, Noda T. Prognosis of replanted primary incisors after injuries. Endod Dent Traumatol. 2000;16(4):175-83.
- Dewhurst SN, Mason C, Roberts GJ. Emergency treatment of orodental injuries: a review. Br J Oral Maxillofac Surg. 1998;36(3):165-75.
- Walker A, Brenchley J. It's a knockout: survey of the management of avulsed teeth. Accid Emerg Nurs. 2000;8(2):66-70.
- Diab M, elBadrawy HE. Intrusion injuries of primary incisors. Part I. Review and management. Quintessence Int. 2000;31(5):327-34.
- Diab M, elBadrawy HE. Intrusion injuries of primary incisors. Part II. Sequelae affecting the intruded primary incisors. Quintessence Int. 2000; 31(5):335-41.
- Dummett CO Jr. Dental management of traumatic injuries to the primary dentition. J Calif Dent Assoc. 2000;28(11):838-45.
- García-Godoy F, Pulver F. Treatment of trauma to the primary and young permanent dentitions. Dent Clin North Am. 2000;44(3):597-632.
- Llarena del Rosario ME, Acosta Alfaro VM, García-Godoy F. Traumatic injuries to primary teeth in Mexico City children. Endod Dent Traumatol. 1992;8(5): 213-4.
- Fried I, Erickson P. Anterior tooth trauma in the primary dentition: incidence, classification, treatment methods, and sequelae: a review of the literature. ASDC J Dent Child. 1995;62(4):256-61.
- Borum MK, Andreasen JO. Sequelae of trauma to primary maxillary incisors. I. Complications in the primary dentition. Endod Dent Traumatol. 1998;14(1):31-44.
- Holan G, Ram D. Sequelae and prognosis of intruded primary incisors: a retrospective study. Pediatr Dent. 1999;21(4):242-7.
- Zilberman Y, Fuks A, Ben Bassat Y, Brin I, Lustmann J. Effect of trauma to primary incisors on root development of their permanent successors. Pediatr Dent. 1986;8(4):289-93.
- MacGregor SA. Management of injuries to deciduous incisors. J Can Dent Assoc. 1969;35(1):26-34.
- von Arx T. Developmental disturbances of permanent teeth following trauma to the primary dentition. Aust Dent J. 1993;38(1):1-10.
- Andreasen JO, Sundström B, Ravn JJ. The effect of traumatic injuries to primary teeth on their permanent successors. I. A clinical and histologic study of 117 injured permanent teeth. Scand J Dent Res. 1971;79(4):219-83.
- Van der Linden F. Some general aspects of the normal development of the dentition. In: Development of the dentition. Chicago: Quintessence Publishing Co; 1983. p. 59-69.
- Sennhenn-Kirchner S, Jacobs HG. Traumatic injuries to the primary dentition and effects on the permanent successors — a clinical follow-up study. Dent Traumatol. 2006;22(5):237-41.
- Ravn JJ. Sequelae of acute mechanical traumata in the primary dentition. A clinical study. ASDC J Dent Child. 1968;35(4):281-9.
- Kramer PF, Zembruski C, Ferreira SH, Feldens CA. Traumatic dental injuries in Brazilian preschool children. Dent Traumatol. 2003;19(6):299-303.
- Turgut MD, Tekçiçek M, Canoglu H. An unusual developmental disturbance of an unerupted permanent incisor due to trauma to its predecessor — a case report. Dent Traumatol. 2006;22(5):283-6.